

Background: Male brow bone reduction almost always requires a bone flap technique for maximal effectiveness. However, it is not the technique of brow bone reduction that is the major consideration in the surgery for men. Rather it is the location of the incision that I find to be the most important consideration which not only affects the access to do the surgery as well as the magnitude of the aesthetic scar tradeoff.
The traditional coronal scalp incision provides the best visibility for removal and replacement of the bone flap in brow reduction. While this is unequivocally true it does not, however, provide the best scar result. The temporal portion of the coronal scalp incision often ends up as potentially the most visible and has the widest scar pattern compared to the part that crosses the top between the bony temporal lines. This is particularly relevant in men with short hair styles or thin hair densities. Given the risk of adverse scarring from such a long scalp incision, it can be a questionable tradeoff in many male brow bone reductions.
Because of this scar risk in men I try to avoid it whenever possible. I prefer to use a more limited scalp incision that stays between the bony temporal lines and avoids transitioning into the vertical temporal scalp areas. In using this approach it is important to understand its limitations. The exposure provided is more like a tunnel and not the wide open exposure provided by a coronal incisional approach. While it provides adequate superior visibility to the brow bones the inferior side cannot be adequately seen until after bone flap removal. It is a more tedious approach and is a bit of a cross between a wide open coronal incision and the very limited access provided by an endoscopic technique.
Two very key points with this limited scalp approach to the brow bones are incision location and frontal hairline pattern. Unlike the coronal incision which is situated way back from the hairline, the limited scalp approach must be either right at the hairline or just behind it. It requires a direct linear line of visibility and can not be behind the curve of the bony forehead as it transitions onto the skull. The frontal hairline pattern will also influence the stretch of the forehead tissues for pocket exposure. The straighter the hairline the better. Men with deep temporal recessed hairlines provide a much more restricted pocket development even though the scar line is longer.

 Case Study: This male requested brow bone reduction. While his frontal hairline had good density with forward projecting hair shafts, it curved way back at the temporal areas.
Case Study: This male requested brow bone reduction. While his frontal hairline had good density with forward projecting hair shafts, it curved way back at the temporal areas.
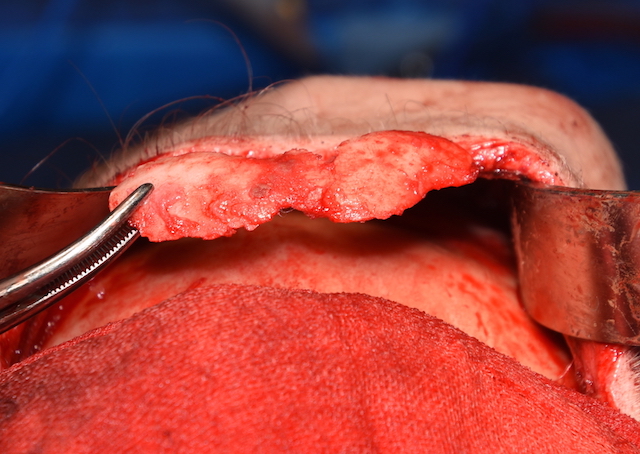
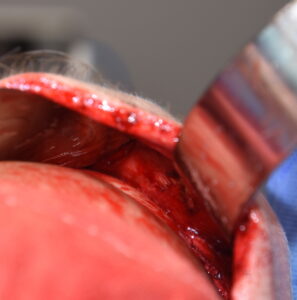 Under general anesthesia an irregular frontal hairline incision was made back to the temporal hairline and stopped before crossing the bony temporal line. The forehead and brow bone soft tissues were elevated and the supraorbital nerves seen as they become evident above the rise of the brow bones. The pocket only permitted a superior ‘tunnel-like’ view of the exposed brow bones.
Under general anesthesia an irregular frontal hairline incision was made back to the temporal hairline and stopped before crossing the bony temporal line. The forehead and brow bone soft tissues were elevated and the supraorbital nerves seen as they become evident above the rise of the brow bones. The pocket only permitted a superior ‘tunnel-like’ view of the exposed brow bones.
 Using a reciprocating saw a one-one-piece bone flap was removed making the cut laying the saw against the forehead above it. Once through the upper and sides of the bone flap osteotomes were used to cut through the inferior portion after which it was removed.
Using a reciprocating saw a one-one-piece bone flap was removed making the cut laying the saw against the forehead above it. Once through the upper and sides of the bone flap osteotomes were used to cut through the inferior portion after which it was removed.

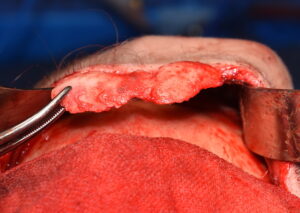
 Interestingly once the bone flap was removed there were only two small openings into the frontal sinus. Additional bone reduction was done along the inferior brow bone rim across the nose to maximize the reduction. Since there were no large frontal sinus exposures the bone flap was not put back. A few pieces of bone from it were used to fill in the two small defects over the frontal sinus.
Interestingly once the bone flap was removed there were only two small openings into the frontal sinus. Additional bone reduction was done along the inferior brow bone rim across the nose to maximize the reduction. Since there were no large frontal sinus exposures the bone flap was not put back. A few pieces of bone from it were used to fill in the two small defects over the frontal sinus.
This male brow bone case brings to light two key issues. First the use of limited frontal hairline incisions can be successful but the pattern of the frontal hairline can make this difficult approach even more so. Secondly, complete bone flap replacement is not necessary if there is only very limited frontal sinus exposure. The less bone that is put back the more significant the brow bone reduction is.
Highlights:
- In the male brow bone reduction patient it is best to avoid, if possible, the typical coronal scalp incision for access.
- The anterior frontal hairline or retro hairline incision provides more limited access for brow bone reduction surgery.
- Complete bone flap replacement in male brow bone reduction may not always be necessary depending upon the contribution of frontal sinus development to the observed external shape.
Dr. Barry Eppley
Indianapolis, Indiana