


Background: Overgrowths of the skull can occur in numerous areas from frontal bossing anteriorly to occipital buns posteriorly. Some have classic appearances and descriptions as in the aforementioned while others are less well known. One of these less well known overgrowths is the elevated or over projecting crown of the head. Somewhat like that of wearing a yamaka or bullcap the crown appears disproportionately high compared to the other convexities of the skull’s shape.
The crown of the head is most commonly used in reference to the scalp and locations of hair loss. When speaking of the skull the crown refers to the vertex beneath the scalp which is the highest point of the top of the head seen in both profile and frontal views. Ir is composed of the paired parietal bones joined by the sagittal suture line. Unlike a sagittal crest, a suture-based bone elevation and a more narrow one, the crown of skull overgrowth is a broader one which is circular in shape and makes the crown appear too high.
Like any patient considering skull reduction the first question is how thick is the bone and how much can be safely reduced. This is where a CT scan is invaluable in most cases to assess the thickness of the skull in the overgrown crown area. What can be safely removed is the outer cortical layer down to the diploic space. In larger skull areas even a few millimeters of reduction makes a visible difference. Significant skull reductions end up creating the need for some scalp reduction as well.
 Case Study: This male was bothered by his high crown skull shape which had a pronounced posterior slope in profile. He desired a crown or vertex skull reduction procedure.
Case Study: This male was bothered by his high crown skull shape which had a pronounced posterior slope in profile. He desired a crown or vertex skull reduction procedure.

 Under general anesthesia and in the supine position the outline of the enlarged crown areas was marked and could be palpated as an elevated ridge at the markings. The scalp incision was marked within the outline of the planned reduced area. Once opened and a wide subperiosteal pocket made full thickness bone cuts were made down into the diploic space in a grid-like pattern to establish the depth of reduction throughout the marked area.
Under general anesthesia and in the supine position the outline of the enlarged crown areas was marked and could be palpated as an elevated ridge at the markings. The scalp incision was marked within the outline of the planned reduced area. Once opened and a wide subperiosteal pocket made full thickness bone cuts were made down into the diploic space in a grid-like pattern to establish the depth of reduction throughout the marked area.
 Then the remaining raised areas of bone between the cut lines was reduced by high speed burring until a continuous smooth surface was obtained. The maximal amount of bone reduced at the thickest central part was 7mms which was the thickness of the rotary burr.
Then the remaining raised areas of bone between the cut lines was reduced by high speed burring until a continuous smooth surface was obtained. The maximal amount of bone reduced at the thickest central part was 7mms which was the thickness of the rotary burr.

 With the skull reduction completed a large amount of excess scalp was evident. To tighten the scalp over the reduced bone area 15mms of scalp was excised centrally and tapered to the sides of the incision so as not to lengthen it. (scalp reduction) Scalp closure was done over a drain with resorbable sutures.
With the skull reduction completed a large amount of excess scalp was evident. To tighten the scalp over the reduced bone area 15mms of scalp was excised centrally and tapered to the sides of the incision so as not to lengthen it. (scalp reduction) Scalp closure was done over a drain with resorbable sutures.

 The drain was removed the following day.The reduction in the height of the crown of his skull was apparent in the profile even with early swelling.
The drain was removed the following day.The reduction in the height of the crown of his skull was apparent in the profile even with early swelling.
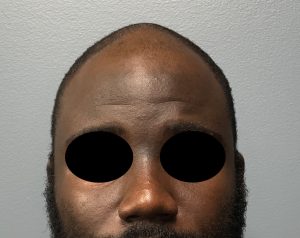
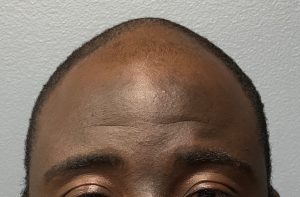
 In the front view the posterior height of the crown area could be seen to be reduced as well.
In the front view the posterior height of the crown area could be seen to be reduced as well.
One might argue that the success of any substantative skull reduction procedure results in scalp excess and the need for scalp removal. That of course depends on how one defines what a substantative skull reduction is as well as what is the thickness and elasticity of the scalp over the reduced area. In many skull reductions the scalp will naturally shrink down provided it is not overly thick and does not have a lot of elasticity to it initially. The need for scalp reduction in skull reductions is more of a consieration in very thick scalps that have a lot of elasticity which is more commonly seen in darker skin pigmented patients.
Key Points:
1) An unaesthetic high crown of the head is associated with an elevated posterior slope in profile and a circumferential bony overgrowth.
2) The crown of the head can be visibly and safely reduced by removal of the thickened outer cortical bone layer. (skull reduction)
3) With substantial bone removal at the crown of the skull some scalp reduction may be needed as well to show the full effects of the reductive changes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon