


Background: The occipital bone is often referred to as the skull bone on the back of the head even though this is not anatomically accurate. It does not make up all the bone on the back of the head even though it makes up a significant part of it. It really only makes up the lower half of the occipital region, part of which is visible (upper half) and part of which is not visible. (lower half below the muscle which encases the spinal cord) With a shallow dish shape it is only the upper half that is seen.
The occipital bone is the thickest of the seven cranial bones which is the result of its primary functions. It protects the brain from back of the head trauma as well as serves as an attachment surface for numerous strong neck muscles. Thus it is no surprise that int s a thick bone with a larger diploic space than other cranial bones.
Protrusions of the occipital bone occur in two types, spot vs global enlargements. The one isolated spot of the occipital bone that can become enlarged is the inion or knob. This small central spike of bone off of the lower edge of the visible occiput produces a distinct knob as its name suggests. Conversely, enlargement of the entire visible occipital bone results in a distinct mound on the back of the head which increases the anteroposterior length of the head and also disrupts a more normal convex shape in profile. It is commonly called a bun as it can look like a hair bun which women out up their hair. While an excessively prominent occipital bone can occur in some genetic disorders, its occurrence is typically idiopathic rather than syndromic.
Both the occipital knob and bun can be reduced but the bun poses bigger challenges in reduction given the extent of its skull’ surface area involvement.
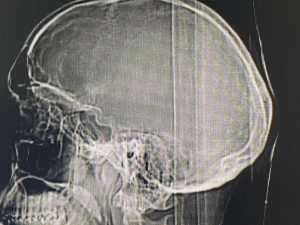 Case Study: This male was bothered by the protrusion on the back of his head which was a classic occipital bun skull protrusion. A side view x-ray shows the occipital bone protrusion which is the result of increased bone thickness.
Case Study: This male was bothered by the protrusion on the back of his head which was a classic occipital bun skull protrusion. A side view x-ray shows the occipital bone protrusion which is the result of increased bone thickness.

 Under general anesthesia and in the prone position a small 6cm horizontal scalp incision was made at the base of the occipital protrusion. Through this incision subperiosteal dissection exposed the entire bony protrusion up to and over the lambdoid sutures.Using a high speed handpiece and burr radiating cuts were made from the incision through the out cortex of the bone to establish maximal depth. Then between the depth lines the bone was removed on sections for an even reduction.
Under general anesthesia and in the prone position a small 6cm horizontal scalp incision was made at the base of the occipital protrusion. Through this incision subperiosteal dissection exposed the entire bony protrusion up to and over the lambdoid sutures.Using a high speed handpiece and burr radiating cuts were made from the incision through the out cortex of the bone to establish maximal depth. Then between the depth lines the bone was removed on sections for an even reduction.
 Over a drain the scalp incision was closed with resorbable sutures in layers.
Over a drain the scalp incision was closed with resorbable sutures in layers.

 The immediate intraoperative results shows the amount of reduction in the back of head protrusion.
The immediate intraoperative results shows the amount of reduction in the back of head protrusion.

 When seen the next day for head dressing and drain removal the reduction change was confirmed in the upright standing position.
When seen the next day for head dressing and drain removal the reduction change was confirmed in the upright standing position.
The first step in evaluating the occipital bun is to get a lateral skull x-ray or a 2D CT scan. It is important to know of the occipital protrusion is due to thicker bone with a normal intracranial bone surface or whether the bone is actually thinner and it is the brain and meninges that is the main component of the protrusion. While I have never seen the latter it is always possible so it is good to make a diagnostic check before surgery. At the least the radiographic assessment will determine how much bone can be removed in millimeters to give the patient an idea of how much reduction of the occipital bun can be achieved.
Case Highlights:
1) Excessive overgrowth of the visible occipital bone creates the bun deformity with a protrusion up to the lambdoid suture lines.
2) The occipital bun skull deformity is the result of bone overgrowth and can be surgically reduced within the limits of the thickness of the outer cortical bone layer of the skull.
3) The small incisional approach to occipital bun reduction surgery is based on incremental bone reduction to create space to reach the outer perimeter of the excessive projection at the lambdoid sutures.
Dr. Barry Eppley
World-Renowned Plastic Surgeon