

Background: There are numerous methods of facial assessment when determining the most aesthetically pleasing facial proportions. One of the most commonly used methods is that of the facial thirds. This is a vertical assessment of the length of the face broken down into 3 sections, frontal hairline to flabella (upper), glabella to central nasal base known as the subnasale (middle) and the subnasale to the bottom of the chin (gnathion) to make up the lower third of the face.
Of the three facial thirds they are not all equally changeable by surgery. The ability to alter the facial thirds by surgery depends how much the bony support underneath it can be changed and whether or how much the overlying soft tissues respond to the alteration of the bony support. In this regard each facial third is very different in their ability to be changed which also varies in whether it is a lengthening or reduction type change.
The one facial third that this is the most surgically responsive to change is the lower third. This is because it is an edge or projecting part of the face as opposed to the other two-thirds of the face which can do little to push up or down on its vertical length because of their attachments. The lower third is unique is that regard as it is ‘free’ on its underside. It also has the advantage that the overlying soft tissues are responsive to the bone changes and almost move 1:1 with it. (more true for lengthening than for shortening)
The greatest aesthetic length increase that can be achieved in the face is vertical chin lengthening, With potential movements of up to 20mms of lengthening their facial reshaping effects can be significant.
Case Study: This male desired a vertically longer chin of some significance. By his own measurements he wanted 15mms of vertical lengthening. A few millimeters of added horizontal projection would be nice but not essential. (per the patient) He regularly thrust or held his jaw forward as he felt that made him look better.
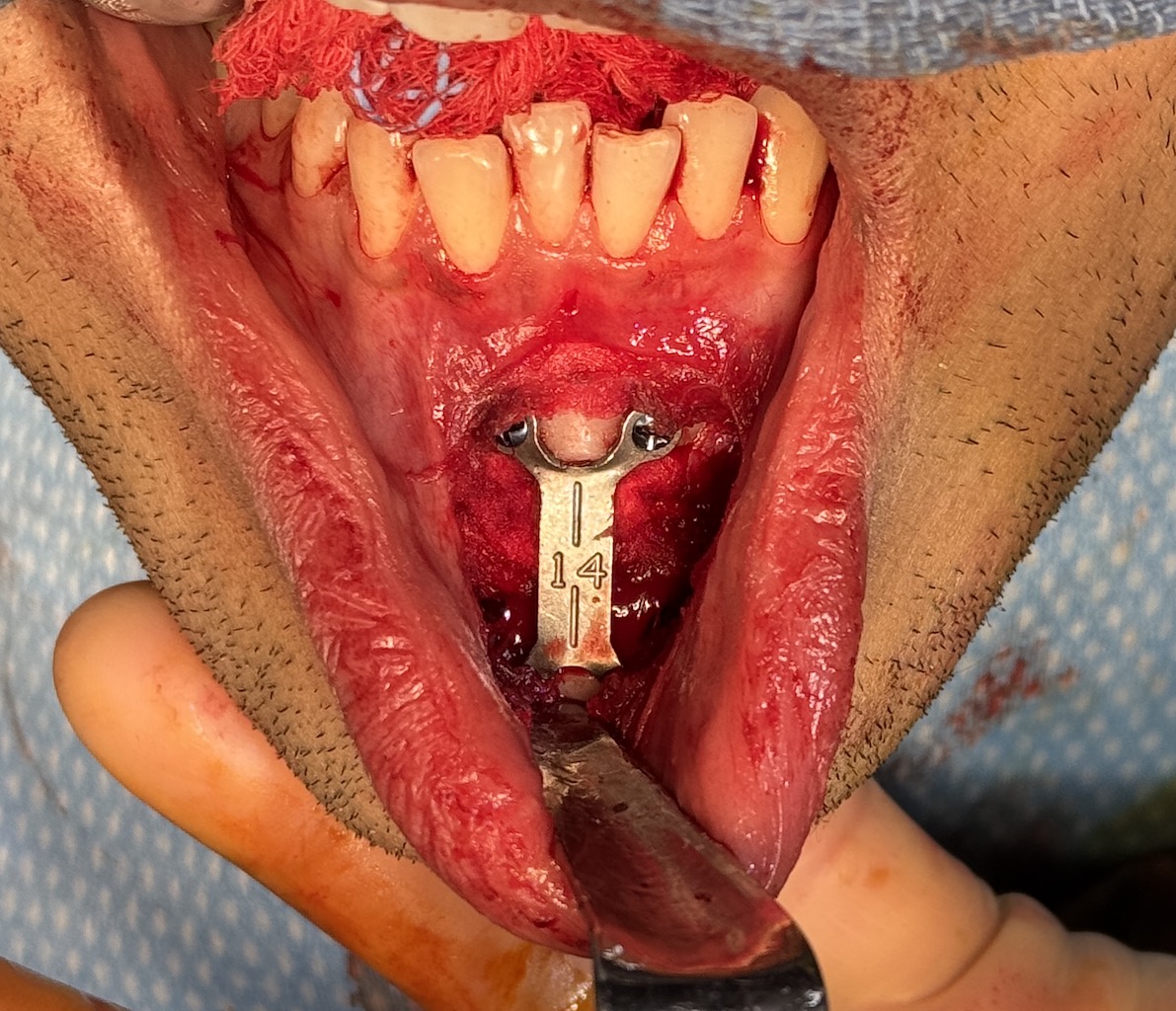
 Under general anesthesia and through an intraoral approach a low horizontal oblique osteotomy was done and the chin dropped down (lengthened) as much as the soft tissues would permit. (14mms) It was held into this position with a 14mm plate and screws. An interpositional cadaveric bone graft was fashioned and placed into the wedge gap.
Under general anesthesia and through an intraoral approach a low horizontal oblique osteotomy was done and the chin dropped down (lengthened) as much as the soft tissues would permit. (14mms) It was held into this position with a 14mm plate and screws. An interpositional cadaveric bone graft was fashioned and placed into the wedge gap.

 His early results showed the dramatic difference in his facial shape with increased vertical length that even made his face look less wide. This two day after surgery result showed swelling and some bruising which will resolve over the next few weeks to look even better.
His early results showed the dramatic difference in his facial shape with increased vertical length that even made his face look less wide. This two day after surgery result showed swelling and some bruising which will resolve over the next few weeks to look even better.

 In side view his once flat mandibular plane angle become more inclined. (chin lower than his jaw angle)
In side view his once flat mandibular plane angle become more inclined. (chin lower than his jaw angle)
Vertical chin lengthening is a powerful facial reshaping procedure in the more square-shaped flat mandibular plane angle patient. Most patients are self-selected because they know their lower facial thirds are short and often do personal maneuvers to help improve it. Some patients like this one present with knowledge of exactly how much vertical lengthening they need by various measurements and/or imaging. While some modest vertical chin lengthening can be achieved with an implant more significant amounts needed to be done by an osteotomy to overcome the soft tissue chin pad restrictions. One aesthetic consideration is that the vertical lengthening chin osteotomy will make the chin look somewhat more narrow.
Key Points
1) The vertically short chin usually creates a face that looks boxy or more square shaped.
2) Patients with short chins are usually well aware of it as they often use jaw posturing to create a more proportionate facial shape.
3) When the amount of vertical chin lengthening needed is greater than 5mms it is best done using a vertical lengthening bony genioplasty with an interpositional bone graft.
Dr. Barry Eppley
World-Renowned Plastic Surgeon