

Background: While the sliding genioplasty can produce a variety of bone movements, its most common dimensional change is horizontal advancement. While the benefits of horizontal bone advancement are seen in the front end of the chin, there are potential liabilities at its back end. As the chin bone is advanced, depending on how much it is moved forward as well as the angulation of the bone cut, a contour deformity can occur at the end of the osteotomy line along the inferior border of the jawline. Known as a notch or step off the smooth inferolateral border of the jawline can develop a contour deficiency seen on the outside as an indentation at the side of the chin.
Stepoff deformities from a sliding genioplasty can be treated by an implant placed over them. Regardless of the implant material it needs to be thin and have fine edging so as to not create another type of palpable or visible edging. The other implant feature that is important is ease of reversibility. Should the implant not be placed ideally or inadequately solves the problem, removing it should not pose another issue.
Case Study: This male had a prior history of a sliding genioplasty which had good projection but bothersome stepoffs at the sides of the chin. They were secondarily treated by the intraoral placement of onlay Medpor implants with screw fixation. Unfortunately their thickness were equally bothersome as the bone defects and he wanted them removed and replaced with a new custom chin implant that adequately and smoothly cover the bone defects.
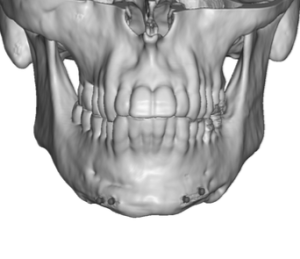
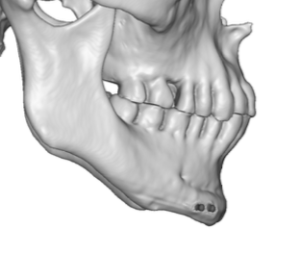 A 3D CT scan showed the chin/jawbone and the screws but not the Medpor implant material. (which is common) The position and size of the Medpor implants had to be presumed but not known before surgery. The screws provided a guide as to how thick the implants were.
A 3D CT scan showed the chin/jawbone and the screws but not the Medpor implant material. (which is common) The position and size of the Medpor implants had to be presumed but not known before surgery. The screws provided a guide as to how thick the implants were.
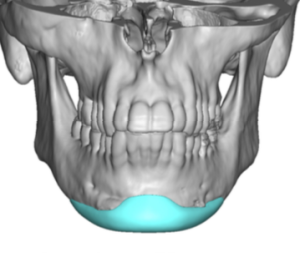
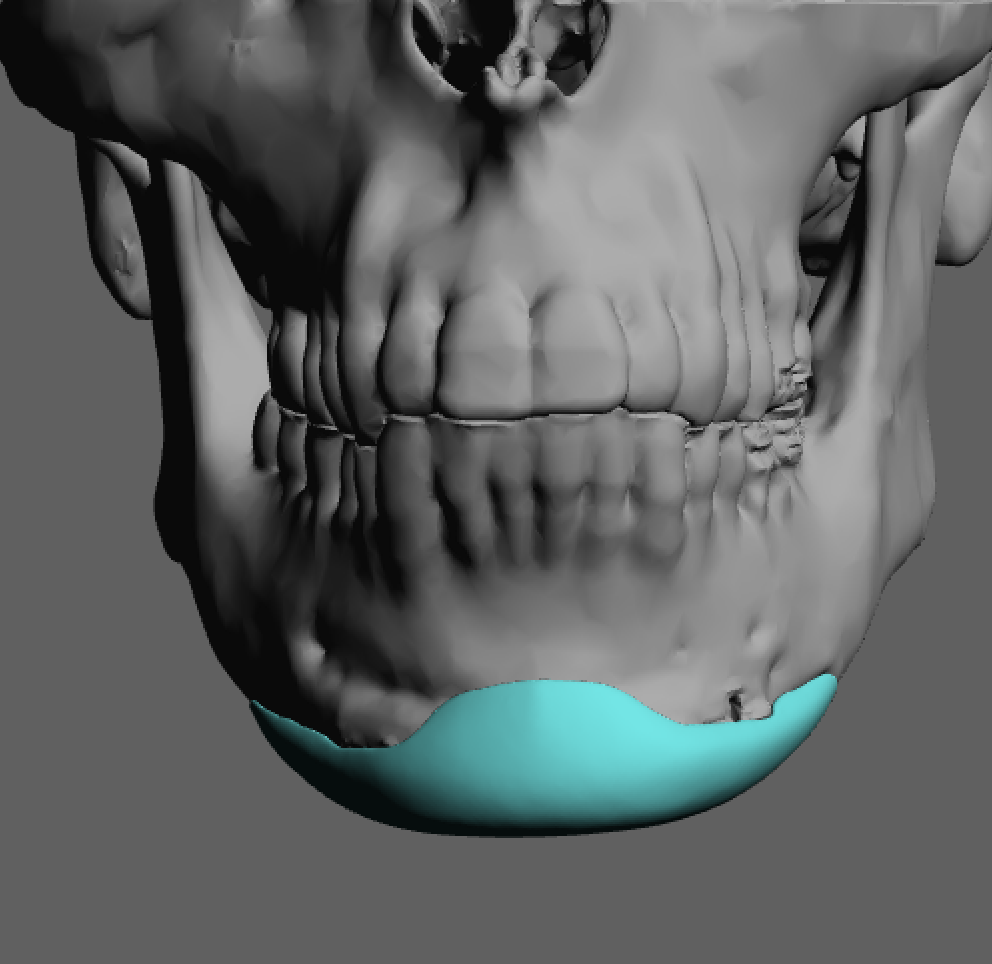
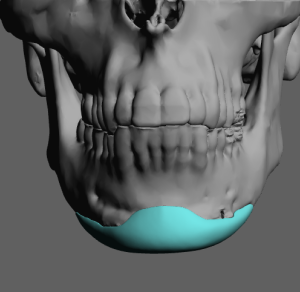
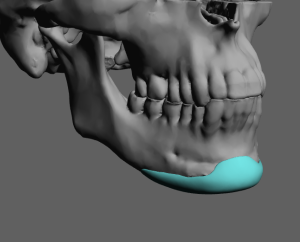
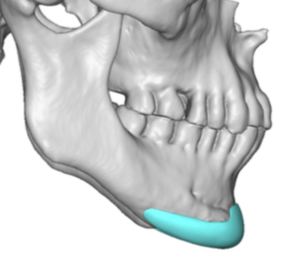 Using the same 3D CT scan a custom chin implant was designed to cover the sliding genioplasty and add a few more millimeters of chin projection. It is more assured that the side implants are in the proper place if the implant design is connected from side to side.
Using the same 3D CT scan a custom chin implant was designed to cover the sliding genioplasty and add a few more millimeters of chin projection. It is more assured that the side implants are in the proper place if the implant design is connected from side to side.

 Under general anesthesia and through his existing intraoral incisions the Medpor implants were identified as side only implants and were likely cut out from an existing Medpor chin implant. In removing Medpor implants one can usually forget about trying to remove the screws by backing them out. The heads of the screws can be stripped and their angulation of placement can make them difficult to remove. The Medpor material is removed from around the screws, usually in a piece meal fashion, and then they can more easily be removed or broken off at the bone surface with their exposed shaft.
Under general anesthesia and through his existing intraoral incisions the Medpor implants were identified as side only implants and were likely cut out from an existing Medpor chin implant. In removing Medpor implants one can usually forget about trying to remove the screws by backing them out. The heads of the screws can be stripped and their angulation of placement can make them difficult to remove. The Medpor material is removed from around the screws, usually in a piece meal fashion, and then they can more easily be removed or broken off at the bone surface with their exposed shaft.
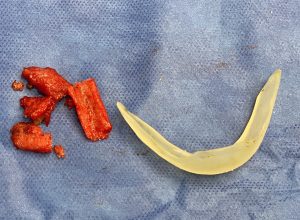
 With the extensive dissection needed to remove the Medpor material the pocket is more than adequately made to place the new custom chin implant.
With the extensive dissection needed to remove the Medpor material the pocket is more than adequately made to place the new custom chin implant.
 The margin of error in recontouring small bone defects along the jawline is very narrow. The most importantly feature of any material to do so needs to be isa ability to create feather edging at the bone transition areas. The other important features are how easily is it to place and remove later if needed. Tissue ingrowth into the material may have is benefits but that material property is way down the list in priority.
The margin of error in recontouring small bone defects along the jawline is very narrow. The most importantly feature of any material to do so needs to be isa ability to create feather edging at the bone transition areas. The other important features are how easily is it to place and remove later if needed. Tissue ingrowth into the material may have is benefits but that material property is way down the list in priority.
Case Highlights:
1) The sliding genioplasty can result in a more narrow chin that some males may dislike.
2) Secondary implant coverage of a lateral sliding genioplasty defect needs to be feather edged to not create a different type of contour deformity.
3) To optimize implant placement and feather edging for jawline contour deformities a custom implant approach is most ideal.
Dr. Barry Eppley
Indianapolis, Indiana