


Background: Since chin reduction is not as commonly requested or performed as chin augmentation the techniques to do so are not often well understood. In the traditional macrogenia female, the reflex operation for most plastic surgeons is an intraoral burring chin reduction technique. It is a reflex operation because the first thought is in how to do it in a scarless manner. While the intraoral approach is scarless and decent results are possible in the properly selected patient, it is a dimensionally limited procedure with a potential for soft tissue issues.
To do an intraoral approach the soft tissue chin pad must be detached from the bone through subperiosteal elevation. This permits the bone to be reduced in the horizontal and width dimensions. (but not vertically) With the closure of the intraoral incision what is not apparent is there is now a loss of bone support and a relative excess of the soft tissue chin pad. While some soft tissue contraction of the chin pad can occur, like in all soft tissues, the chin pad is unique because it is stretched out tissue over a projection point. Thus when it contracts it tends to ball up rather than lay completely flat/smooth. This can result in a chin pad ptosis with fullness off the end of the chin bone that is magnified when one smiles.
Correcting soft tissue chin pad excess/ptosis is not usually effective done by intraoral resuspension. It may help somewhat by you can’t lift away or resuspend soft tissue excess. Again the intraoral approach is appealing but that should not be confused with effectiveness.

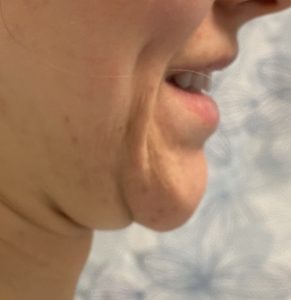 Case Study: This female had a prior history of an intraoral burring chin reduction which resulted in a wider fuller chin. It was treated secondarily by an intraoral suspension technique which did not make much improvement. She wanted the soft tissue chin pad reduced/tightened and some additional vertical chin shortening.
Case Study: This female had a prior history of an intraoral burring chin reduction which resulted in a wider fuller chin. It was treated secondarily by an intraoral suspension technique which did not make much improvement. She wanted the soft tissue chin pad reduced/tightened and some additional vertical chin shortening.

 A submental approach was undertaken with an excisional area marked out using a natural skin crease for the initial incision at the neck side of the excision. The soft tissue chin pad was elevated off of the bone and 2mm of the inferior border of the chin vertically reduced. With this bony reduction comes a difference in the levels of the front and back edges of the excision.
A submental approach was undertaken with an excisional area marked out using a natural skin crease for the initial incision at the neck side of the excision. The soft tissue chin pad was elevated off of the bone and 2mm of the inferior border of the chin vertically reduced. With this bony reduction comes a difference in the levels of the front and back edges of the excision.
 The mentalis muscle of the soft tissue chin pad was then sewn onto the underside of the chin bone to the periosteal edge. Redundant skin and fat was excised from the soft tissue pad and then closed to the incisional edge in the neck. Any residual submental fullness below the inciseon was treated by small cannula liposuction.
The mentalis muscle of the soft tissue chin pad was then sewn onto the underside of the chin bone to the periosteal edge. Redundant skin and fat was excised from the soft tissue pad and then closed to the incisional edge in the neck. Any residual submental fullness below the inciseon was treated by small cannula liposuction.

 Her intraoperative result showed what the original objective was for the soft tissue chin pad reeshaping/tightening…getting a better match between the overlying soft tissue and the underlying bone.
Her intraoperative result showed what the original objective was for the soft tissue chin pad reeshaping/tightening…getting a better match between the overlying soft tissue and the underlying bone.
Case Highlights:
1) An intraoral chin reduction can result in soft tissue chin pad ptosis due to loss of bone support and periosteal attachments
2) Attempts at intraoral chin pad resuspension frequently fail as a major component of the problem is a now excessive soft tissue chin pad where some reduction is needed.
3) The submental approach allows for a combination of redundant tissue excision and chin pad tissue tightening.
Dr. Barry Eppley
Indianapolis, Indiana