


Background: The skull is simplistically a collection of five almost flat to very convex surfaces. All of these skull surfaces usually have smooth outer contours but are prone to a wide variety of possible irregularities from either congenital, traumatic or pathologic origins. A significant number of such surface contour irregularities are related to the suture lines that connect the skull bones as they impact its growth and connectivity.
But there some surface contour changes that do not relate to sutural connections and skull plate growth One unique type of a bony prominence or outgrowth is the occipital knob or inion which occurs at the center of the nuchal ridge line on the back of the head. This solitary bony prominence can vary in size but its prominence can be accentuated if the skull above it lacks normal projection, creating a reverse slope rather than a convex shape in profile.
Indentations of the skull often come from traumatic injuries and less commonly from congenital origins…unless the two are linked. One possible link is forceps delivery where a circular indent can be created during the birth process. This causes a very specific circular indentation that is present at birth and remains throughout the patient’s life.
The wide or excess convexity to the side of the head is uniquely different from all other skull contour concerns because it is soft tissue and not bony-based. The temporal muscle contributes more to the width of the side of the head than the bone particularly at its anterior portion. Subtotal muscle removal is a very effective method of head width reduction and does not cause any functional issues.
But if all of these skull contour issues occur in the same patient (occipital knob, flat back of the head, circular skull indentation and a wide head) can they be simultaneously treated in a single surgery?
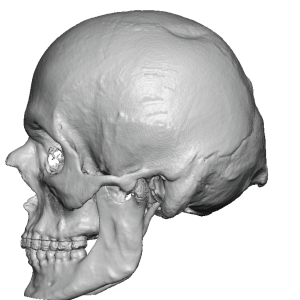
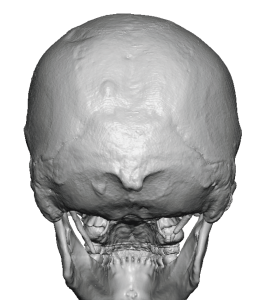 Case Study: This male had all of the above noted skull contour issues, three of which were visible on his 3D CT scan due to their bony nature. (occipital knob, .flat back of head and circular indent)
Case Study: This male had all of the above noted skull contour issues, three of which were visible on his 3D CT scan due to their bony nature. (occipital knob, .flat back of head and circular indent)
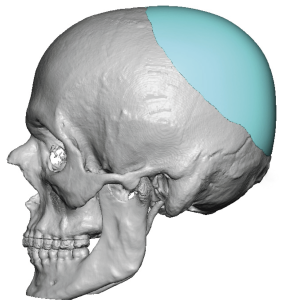
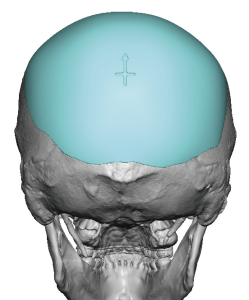 To address the flat back of the head and fill in the circular indentation a custom skull implant was designed. On the scan the occipital knob was also digitally reduced as part of the surgical plan.
To address the flat back of the head and fill in the circular indentation a custom skull implant was designed. On the scan the occipital knob was also digitally reduced as part of the surgical plan.
 Under general anesthesia and in the prone position a small horizontal scalp incision was made through which the occipital knob was initial reduced. ( a lap sponge is needed around the incision to protect the hair during high speed burring)
Under general anesthesia and in the prone position a small horizontal scalp incision was made through which the occipital knob was initial reduced. ( a lap sponge is needed around the incision to protect the hair during high speed burring)

 Through the same incision the custom skull implant was placed going in the superior direction. The scalp incision was then closed.
Through the same incision the custom skull implant was placed going in the superior direction. The scalp incision was then closed.
 Staying in the prone position temporal muscle reductions were done through postauricular incisions. Drains were placed that extended back into the implant area as well.
Staying in the prone position temporal muscle reductions were done through postauricular incisions. Drains were placed that extended back into the implant area as well.
The skull’s five surfaces are all prone to contour malformations from bony prominences and indentations to muscle hypertrophy. All five skull surfaces can be treated in a single surgery, the only question is surgical access. Like any single surface aesthetic skull surgery one of the goals is to limit visible scarring. As seen in this case five surgical sites were treated by a single ‘visible’ incision. (the ones behind the ears are never seen) Only in reconstructive or pediatric craniofacial surgery is a bicoronal scalp incision used to perform skull contouring surgery.
Key Points:
1) Multi surface area skull reshaping often consists of a combination of reductions and augmentations.
2) The flat back of the head can be associated with a prominent occipital knob for which implant augmentation and knob reduction can be concurrently performed.
3) Dents in the skull are uncommon when not associated with a traumatic event but can be leveled out with an implant regardless of its cause.
Dr. Barry Eppley
World-Renowned Plastic Surgeon