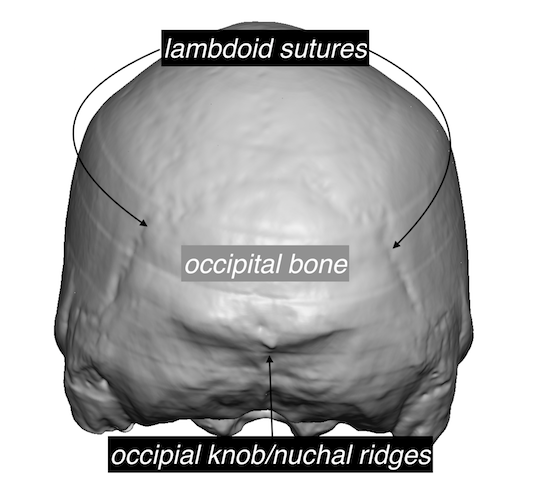


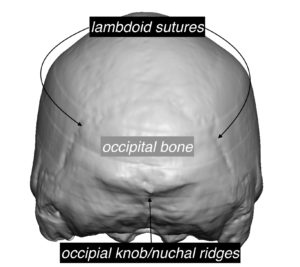
 Background: The back of the head is composed of the occipital bone inferiorly and the parietal bone superiorly. While the back of the head is commonly referred to as the occiput, this anatomically only refers to the lower half of the back of he head. Because of the two different bones that make up the back of the head an their shapes, they are connected by two different suture systems, the superior midline sagittal and the more inferior paired lambdoidal sutures.
Background: The back of the head is composed of the occipital bone inferiorly and the parietal bone superiorly. While the back of the head is commonly referred to as the occiput, this anatomically only refers to the lower half of the back of he head. Because of the two different bones that make up the back of the head an their shapes, they are connected by two different suture systems, the superior midline sagittal and the more inferior paired lambdoidal sutures.
Because the bony anatomic makeup is more complex than most realize, multiple types of aesthetic posterior head shape deformities can occur. One such deformity is occipital bone protrusion. This is where the occipital bone has grown out further than the more superior parietal bone. This creates a classic protrusion that sticks out in profile from the parietal bone above it and stops at the lambdoidal suture line superiorly. The occipital knob and nuchal ridge prominences is also part of the overall occipital bone overgrowth.
An occipital bony protrusion should be differentiated from an occipital knob skull deformity. While they are treated similarly (bone burring reduction) the occipital knob is a smaller midline protrusion that occurs at the bottom edge of the visible occipital bone. In essence it is a mini occipital protrusion.

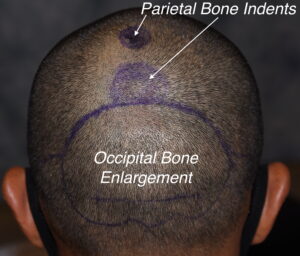 Case Study: This male presented with an occipital bone protrusion that involves all of the visible occiput between the lambdoidal sutures and the nuchal ridges. It had a protrusion of about 6 to 7mms at its thickest portion. The midline occipital knob and the side wing nuchal ridge protrusions could be seen.
Case Study: This male presented with an occipital bone protrusion that involves all of the visible occiput between the lambdoidal sutures and the nuchal ridges. It had a protrusion of about 6 to 7mms at its thickest portion. The midline occipital knob and the side wing nuchal ridge protrusions could be seen.
 Under general anesthesia in the prone intraoperative position a 6.5cm long horizontal irregular scalp incision was made paralleling the direction of the hair shafts from the skin. After subperiosteal underlining of the entire back of the head, the bulging occipital bone could be seen right up to the lambdoid suture line.
Under general anesthesia in the prone intraoperative position a 6.5cm long horizontal irregular scalp incision was made paralleling the direction of the hair shafts from the skin. After subperiosteal underlining of the entire back of the head, the bulging occipital bone could be seen right up to the lambdoid suture line.

 Using a high speed handpiece and a carbide burr vertical and horizontal linear cuts were made through the occipital bone protrusion down to the diploic space. These lines created four quadrants of bone that could be sequentially burred down to allow for an even and smooth reduction.
Using a high speed handpiece and a carbide burr vertical and horizontal linear cuts were made through the occipital bone protrusion down to the diploic space. These lines created four quadrants of bone that could be sequentially burred down to allow for an even and smooth reduction.
 Once the occipital bone was reduced a vertical parietal indentation was seen at the midline where it joined with the lambdoid suture junction. Bone grafting of the indentation was done by creating a putty-like mixture of the bone dust and forming a shape that was onlayed onto the indented parietal bone area.
Once the occipital bone was reduced a vertical parietal indentation was seen at the midline where it joined with the lambdoid suture junction. Bone grafting of the indentation was done by creating a putty-like mixture of the bone dust and forming a shape that was onlayed onto the indented parietal bone area.

 When seen the next day to remove his drain, the improvement in the profile shape of the back of his head could be appreciated.
When seen the next day to remove his drain, the improvement in the profile shape of the back of his head could be appreciated.
The aesthetic success of occipital bone prominence reduction is a small scalp incision and a systematic approach to the bone reduction to ensure an adequate and smooth bone shape. While the limited scalp incision makes it challenging good scalp retraction and a grid pattern approach to the bone reduction ensure optimal results.
Case Highlights:
1) Occipital bony protrusion involves the lower half of the back of the head from the lambdoid suture down to the nuchal ridge.
2) The grid pattern approach to the bone reduction allows for an even reduction of an occipital protrusion through the smallest possible scalp incision.
3) Parietal indentations above the lambdoid suture can be augmented by a bone putty mixture from the reduced occipital bone shavings.
Dr. Barry Eppley
Indianapolis, Indiana