

Background: The most significant topographic feature of the back of the head are the nuchal lines. (nuchal meaning nape of the neck) The nuchal lines are a set of four horizontal fine ridges of bone that exist on the external surface of the occipital bone. The highest nuchal line, known as the Mempin line, is the attachment of the epicranial aponeurosis which extends anteriorly all the way to the brow bones of the forehead. The superior nuchal line lies below it onto which fibers of the trapezius, occipitals and splenius capitis muscles. There are two additional nuchal lines below the superior one but they are on the undersurface of the occipital bone and have no external visibility.
Various enlargements or existoses of the superior nuchal line can occur due to the strong neck muscle attachments to it. This are primarily seen in men given their stronger and thicker neck muscles. Occipital knobs are a midline ball of enlarged bone whose angle off of the occipital bone determines whether it is externally visible. Enlargement of the superior nuchal line presents as a wing-shaped prominent ridge. These occipital protuberances are usually seen as separate entities although rarely can occur together. These enthesophytes are a response to the mechanical stress (muscle strain) placed on them.
There is some suggestion that such occipital bony exostoses are becoming more prominent in younger people. As many as 40% percent of adults examined had bony ‘spurs’ on the back of their head which was postulated due to the contemporary use of hand held devices. I can to speak to this unsubstantiated claim. But what is clear is that short hairstyles and shave heads is making any amount of bony prominences more visible which explains the preponderance of men seeking surgical removal.
 Case Study: This male was bothered by a very prominent bump in the midline of the back of his head that also had prominent raised ridges extending out from the sides of it. This was bothersome both aesthetically as well as caused some discomfort.
Case Study: This male was bothered by a very prominent bump in the midline of the back of his head that also had prominent raised ridges extending out from the sides of it. This was bothersome both aesthetically as well as caused some discomfort.



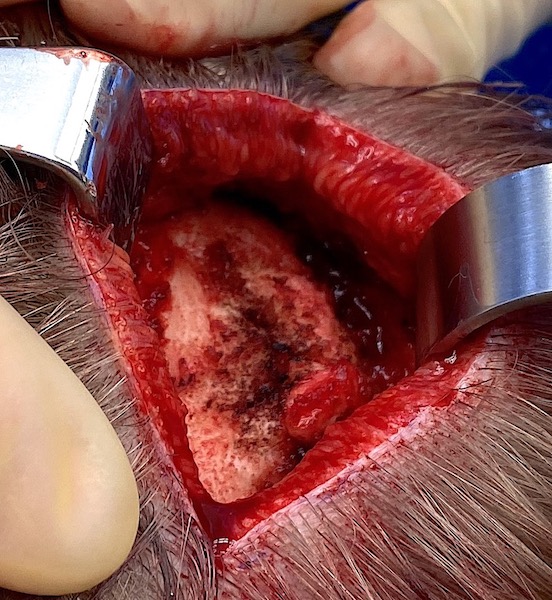
 Under general anesthesia and in the prone position a 7.5cm horizontal scalp incision was made directly over it. Two large paired knobs of bone were encountered with a slight cleft between them. Raised ridges of bone extended out from them along the bottom of the visible occipital bone. Muscle releases were necessary exposed the inferior extent of the bony prominences for adequate reduction. A high speed handpiece and burr was used to reduce them in their entirely from the midline out laterally. Scalp closure was done over a drain.
Under general anesthesia and in the prone position a 7.5cm horizontal scalp incision was made directly over it. Two large paired knobs of bone were encountered with a slight cleft between them. Raised ridges of bone extended out from them along the bottom of the visible occipital bone. Muscle releases were necessary exposed the inferior extent of the bony prominences for adequate reduction. A high speed handpiece and burr was used to reduce them in their entirely from the midline out laterally. Scalp closure was done over a drain.

 The before and after changes were immediately seen for a smooth convex lower occipital bone contour.
The before and after changes were immediately seen for a smooth convex lower occipital bone contour.
There is no question that these lower occipital bony prominences occur much more commonly in men. I have yet to see a female who has presented for their removal. Why they occur in some men and not others in not clear. Nor why they would occur in larger amounts in some patients than others is also not clear. Most come from their removal because of their aesthetic appearance, a few for that as well as some discomfort than comes from them. Complete surgical removal is always possible.
Case Highlights:
1) The muscular attachment region of the occipital bone on the back of the head can create a variety of bony exostoses along the nuchal ridge.
2) The nuchal ridge prominence is distinguished from that of the occipital knob because of its horizontal orientation.
3) Nuchal ridge bony prominences can be completely removed (nuchal ridge skull reduction) with the technical note that muscle release has to be done to adequately get to their underside.
Dr. Barry Eppley
Indianapolis, Indiana