


Background: The skull generally has a smooth convex shape of various arcs on its five surfaces. Abnormal and unaesthetic bony prominences do occur and are often associated along the lines of the sutures due to developmental bony overgrowth. The sutures are active sites of bone formation in the early years and the interplay between the pressure of the expanding brain and the fibrous tissues of the suture account for overall skull size increase.
One of the interesting suture sites on the developing skull is at the anterior and posterior fontanelles. These bony gaps known as ‘soft spots’ are present in every infant and functionally are what makes it possible for the fetal head to pass through the birth canal. Everyone knows the two major fontanelles, the anterior and posterior, of which the posterior one closes first. The anterior fontanelle is the largest of all six of the fontanelles. Because of its size and the need to remain open for brain growth the anterior fontanelle closes last at between 9 and 18 months.
The closure pattern of the anterior and posterior fontanelles can result in two types of associated skull contour deformities. If insufficient bone forms during closure a contour depression can occur because the bone is thinner the the surrounding skull. This is most commonly seen at the posterior fontanelle with a resultant posterior sagittal dip at the crown area. Conversely if excessive bone formation occurs during closure thicker skull area is formed creating a rounded prominence. In my experience this occurs more often at the anterior fontanelle than at the posterior fontanelle.
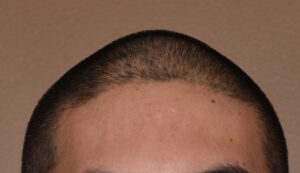
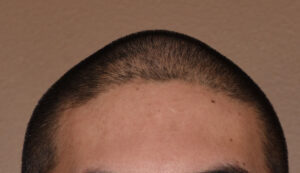
 Case Study: This male presented with a large rounded prominence behind the frontal hairline which had been present as long as he could remember. From the frontal view it created a peaked head shape and from the side view it appeared as an anterior rounded prominence.
Case Study: This male presented with a large rounded prominence behind the frontal hairline which had been present as long as he could remember. From the frontal view it created a peaked head shape and from the side view it appeared as an anterior rounded prominence. 
 Under general anesthesia a small 4cm scalp incision was made at the back end of the bony prominence. After exposing the skull’s surface it could be seen that the thickest part of the prominence was at the confluence of the sagittal and bilateral coronal sutures. A high speed burring reduction technique was done using a tunnel technique with the reduction of a large amount of bone dust. The bony reduction was done centrally and feathered out to the sides. Prior to scalp closure a drain was placed.
Under general anesthesia a small 4cm scalp incision was made at the back end of the bony prominence. After exposing the skull’s surface it could be seen that the thickest part of the prominence was at the confluence of the sagittal and bilateral coronal sutures. A high speed burring reduction technique was done using a tunnel technique with the reduction of a large amount of bone dust. The bony reduction was done centrally and feathered out to the sides. Prior to scalp closure a drain was placed.

 His intraoperative result showed age amount of bony prominence achieved.
His intraoperative result showed age amount of bony prominence achieved.
 His head dressing and drain were removed the next morning where the similar result obtained could also be seen.
His head dressing and drain were removed the next morning where the similar result obtained could also be seen.
 Bony skull prominence reductions can be adequately reduced in most cases. The challenge is to be able to do so through the smallest possible scalp incision for the obvious aesthetic reason. This is not as easy as it may appear due to visualization inside a narrow sub periosteal tunnel. But with time and persistence a significant amount of outer cortical bone can be removed.
Bony skull prominence reductions can be adequately reduced in most cases. The challenge is to be able to do so through the smallest possible scalp incision for the obvious aesthetic reason. This is not as easy as it may appear due to visualization inside a narrow sub periosteal tunnel. But with time and persistence a significant amount of outer cortical bone can be removed.
Case Highlights:
1) The anterior sagittal skull prominence occurs at the confluence of the sagittal and coronal sutures and represents an overgrowth of the anterior fontanelle closure during infancy.
2) A small scalp incision can be used to burr down the bony prominence for a more normal skull shape in both side and frontal views.
3) The recovery from such a skull prominence reduction is rapid with minimal discomfort and upper facial swelling.
Dr. Barry Eppley
Indianapolis, Indiana