

Background: Alloplastic chin augmentation is done most commonly using either a silicone or porous polyethylene implant (Medpor) materials. Each has their own advantages and disadvantages and surgeons have their own preferences. The argument for the use of a silicone implant is that it is to remove/replace if desired. The argument for a Medpor implant is that it gets tissue ingrowth and has no risk of shifting after surgery.
While tissue growth is a seemingly great feature of any implant material, that is a benefit that is most relevant if the implant is never going to be removed. The reality is that the rate of facial implant removal/replacement/adjustment is not low. In this circumstance tissue ingrowth is a disadvantage.
I have read and been told that it is very difficult or impossible remove a Medpor facial implant. Having removed hundreds of them in their entirety their removal is clearly possible and it can be safely done with careful technique..
Case Study: This young male had a history of a prior Medor chin implant placement. While it provided some chin augmentation improvement it was not enough in both projection nor achieved the more square chin shape that he desired.

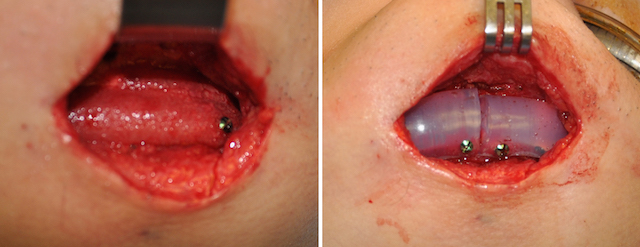
 Under general anesthesia and through his well healed submental chin incision, the Medpor chin implant was removed in its entirety in an ‘inner-outer’ technique. It was replaced by a split square silicone chin implant that was secured by several small screws.
Under general anesthesia and through his well healed submental chin incision, the Medpor chin implant was removed in its entirety in an ‘inner-outer’ technique. It was replaced by a split square silicone chin implant that was secured by several small screws.
The best and safest way to remove any Medpor facial implant is with what I call the ‘inner-outer’ technique. This is where the implant is initially separated from the bone on its underside. It is no problem getting between the implant and the bone as I have yet to see any bone ingrowth into the material, there is always a softvtissue capsule between the implant and the bone. This separation can be developed completely and easily with no risk of injury to any surrounding structures. Once the implant segment has some mobility needle tip electrocautery is used carefully on the outer surface to release the firmly fixed overlying soft tissue. It is important to hang onto the implant and pull it towards the incision as it gets free, moving the very thin tail out of the long tissue tunnel. Sometimes the thin tail breaks off but it must be retrieved to avoid a residual bump along the jawline.
Case Highlights:
1) Medpor chin implants commonly have very long wings and are secured with multiple screws.
2) The removal of Medpor chin implants requires that the thin tails are completely removed far away from the incision.
3) The complete removal of a Medpor chin implant creates an adequate for the replacement of a new chin implant if desired.
Dr. Barry Eppley
Indianapolis, Indiana