

Background: The historic and still commonly performed method of lower jaw augmentation is with the use of standard chin and jaw angle implants. Three in dependently placed implants on the bony corners of the lower face can effectively create a more visible or defined jawline. Barring any complications many implanted patients go on to live with their jaw implants forever. But some patients, even with initially satisfying results, may eventually think about improvements and the consideration of a connected jawline implant that provides increased dimensions is the only option moving forward.
All connected jawline implants are custom designed from a. 3D CT scan. From the scan the existing implants can be seen with their shapes and position on the bone. (unless it is Medpor material which can’t be seen) Often changes of the bone around the implant will be seen consisting of varying amounts of overgrowth. While this is well known to occur around chin implants, it is not usually appreciated that it occurs around jaw angle implants as well. This biologic response is to be expected since the implants are placed in the subperiosteal location.
When replacing jaw implants it is always necessary to remove these bone overgrowths. For some of them it is necessary to remove them to get the implants out. But for all of them they need to be removed/smoothed out so the new implant lies as flat as possible on the jawbone.
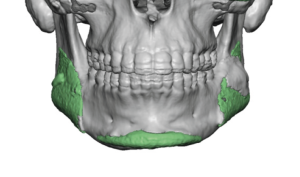
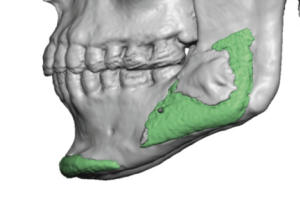 Case Study: This male has a prior history of standard chin and jaw angle implants placed which produced a satisfactory result. A large bone overgrowth had developed over the left jaw angle implant while the chin implant has some edge overgrowth. Due to having some other procedures seven years later he decided to replace his standard jaw implants with a custom wrap around jawline implant.
Case Study: This male has a prior history of standard chin and jaw angle implants placed which produced a satisfactory result. A large bone overgrowth had developed over the left jaw angle implant while the chin implant has some edge overgrowth. Due to having some other procedures seven years later he decided to replace his standard jaw implants with a custom wrap around jawline implant.
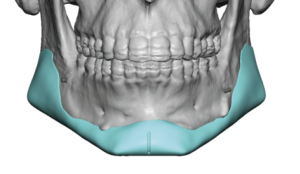
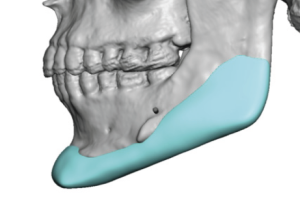 The goal of the new jawline implant was to add a few millimeters to what the current chin and jaw angle implants had achieved and to then make it all connected as a single implant.
The goal of the new jawline implant was to add a few millimeters to what the current chin and jaw angle implants had achieved and to then make it all connected as a single implant.

 Under general anesthesia and through his existing submental and intraoral scars, his chin and jaw angle implants were removed along with a large bone overgrowth. The capsule on the bone was lifted up and displaced superiorly to allow the jawline implant to be placed.
Under general anesthesia and through his existing submental and intraoral scars, his chin and jaw angle implants were removed along with a large bone overgrowth. The capsule on the bone was lifted up and displaced superiorly to allow the jawline implant to be placed.
When it come to replacing existing jaw implants with new ones this secondary surgery is always harder than the placement of the first implants where no such biologic tissue reactions have developed. The combination of scar (capsule) and bone overgrowths makes the dissection more difficult. The key is to go get under the existing capsule and lift it off the bone and push it outward. (capsular displacement) There is very little working room to try and remove get capsule due to the small incisional work space. This will also provide a clear view of any residual bone overgrowths that need to be removed.
 When it comes to bone overgrowths at the chin and jaw angles, there is usually a more robust bone deposition at the jaw angles. In some cases, if you don’t have a preoperative 3D CT scan, the bone overgrowth hides the implant and initially one can not seem to find it. This bone overgrowth occurs superiorly at the thickest part of the muscle. The raised periosteum acts a nidus for bone formation which uses the smooth implant surface as a platform on which to spread. To no surprise the thick masseter muscle is a bigger stimulus than the smaller muscles of the chin.
When it comes to bone overgrowths at the chin and jaw angles, there is usually a more robust bone deposition at the jaw angles. In some cases, if you don’t have a preoperative 3D CT scan, the bone overgrowth hides the implant and initially one can not seem to find it. This bone overgrowth occurs superiorly at the thickest part of the muscle. The raised periosteum acts a nidus for bone formation which uses the smooth implant surface as a platform on which to spread. To no surprise the thick masseter muscle is a bigger stimulus than the smaller muscles of the chin.
Case Highlights:
1) Some standard chin and jaw angle implants patients ‘graduate’ to a custom jawline implant for an enhanced and linear jawline look.
2) While chin implants are well known to develop varying amounts of thin edge bony overgrowths, jaw angle implants can develop much more profound bony overgrowths over their superior edges.
3) Replacing existing chin and jaw angle implants with a total coverage jawline implant requires removal of all bony overgrowths and elevation of the existing capsule.
Dr. Barry Eppley
Indianapolis, Indiana