


Background: While chin augmentation is a commonly performed facial reshaping procedure, there are some basic concepts about it that can be overlooked. First, there are gender differences between what the ideal chin position may be. Too often this is overlooked in women who are far more likely to end up over corrected than under corrected. Secondly, in very deficient female chins postoperative accommodation to the change can be sometimes challenging. It serves everyone well to do preoperative computer imaging to see what the potential accommodation change amount is.
In very short chins the sliding genioplasty has several advantages over a chin implant particularly in a female. When the chin is significantly short it is angled backwards. Placing an implant on an incline loses some of its intended horizontal augmentation effect but, more importantly, creates undesired vertical elongation. There is nothing a standard chin implant can do to prevent that change because of the platform that it sits on. A sliding genioplasty moves the angled chin bone forward and up obviating any lengthening effect.
The sliding genioplasty in the very short chin also has an improved effect on the neck beyond what an implant can do. By moving the chin bone forward it pulls the upper neck muscles that are attached to it. This not only lengthens the anterior bony jawline but stretches out the muscle and soft tissues that make up the submental neck region further enhancing the neckline. When this is combined with submental liposuction the maximal neck reshaping effect is created.
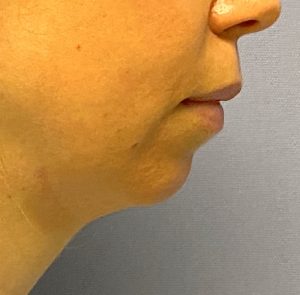
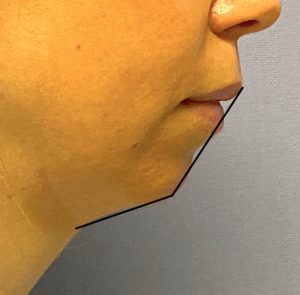 Case Study: This female desired to improve a congenitally short chin that had bothered her lifelong. She had a significantly recessive chin as defined by a linear measurement (16mm horizontal deficiency as measured from a vertical line dropped down from the lower lip) as well as a very obtuse cervicomental angle. The combination of computer imaging and preoperative measurements determined that the acceptable amount of forward chin movement was 8mms with no vertical elongation.
Case Study: This female desired to improve a congenitally short chin that had bothered her lifelong. She had a significantly recessive chin as defined by a linear measurement (16mm horizontal deficiency as measured from a vertical line dropped down from the lower lip) as well as a very obtuse cervicomental angle. The combination of computer imaging and preoperative measurements determined that the acceptable amount of forward chin movement was 8mms with no vertical elongation.
 Under general anesthesia and through a limited intraoral vestibular incision the chin bone was fully exposed. Low angled long osteotomy bone cuts were made 5mms below the mental foramen and the chin segment downfractured. Using a bent 8mm set plate the chin was advanced in its new position with it angled upwards 2mms to prevent any vertical lengthening.
Under general anesthesia and through a limited intraoral vestibular incision the chin bone was fully exposed. Low angled long osteotomy bone cuts were made 5mms below the mental foramen and the chin segment downfractured. Using a bent 8mm set plate the chin was advanced in its new position with it angled upwards 2mms to prevent any vertical lengthening.
 In the congenitally very short chin even an 8mm advancement will put the back edge of the advanced chin bone at the front edge of the superior chin segment. It is most ideal to maintain some central bone contact between the two bone segments but not critical as the wings or side of the mobilized chin bone will always have contact
In the congenitally very short chin even an 8mm advancement will put the back edge of the advanced chin bone at the front edge of the superior chin segment. It is most ideal to maintain some central bone contact between the two bone segments but not critical as the wings or side of the mobilized chin bone will always have contact
 With a large step off between the two chin segments I prefer to bone graft the new abnormal shape of the chin with cadaveric bone chips. This helps restore the normal convex profile of the chin which will soften the deepening effect on the overlying labiomental fold and lower the risk of lower lip tightness.
With a large step off between the two chin segments I prefer to bone graft the new abnormal shape of the chin with cadaveric bone chips. This helps restore the normal convex profile of the chin which will soften the deepening effect on the overlying labiomental fold and lower the risk of lower lip tightness.
Submental liposuction was then performed to improve the shape of the chin advancement. (sharpen the cervicomental angle)

 Her intraoperative results showed the significant but not overdone change in her lower facial profile. This looked very much like the preoperative computer imaging.
Her intraoperative results showed the significant but not overdone change in her lower facial profile. This looked very much like the preoperative computer imaging.

 Chin augmentation is an interesting type of facial reshaping surgery whose patient satisfaction level goes beyond just a well placed chin implant or a technically sound sliding genioplasty. No matter how much a patient desires a change how well they can accept the difference in their appearance is not assured. This is no better seen than in the female whose has had a lifelong short chin. I have seen many a female patient who presents for a chin augmentation revision because the change has been too great whether it is an implant or a bone movement. It may look completely fine to the surgeon who performed it or to others, or may even look ideal compared to a numerical or angle standard, but the patient does not feel comfortable because they do not recognize themselves. Usually no preoperative computer imaging has been done and the patient understandably left it up to the surgeon’s judgment as to what looks best.
Chin augmentation is an interesting type of facial reshaping surgery whose patient satisfaction level goes beyond just a well placed chin implant or a technically sound sliding genioplasty. No matter how much a patient desires a change how well they can accept the difference in their appearance is not assured. This is no better seen than in the female whose has had a lifelong short chin. I have seen many a female patient who presents for a chin augmentation revision because the change has been too great whether it is an implant or a bone movement. It may look completely fine to the surgeon who performed it or to others, or may even look ideal compared to a numerical or angle standard, but the patient does not feel comfortable because they do not recognize themselves. Usually no preoperative computer imaging has been done and the patient understandably left it up to the surgeon’s judgment as to what looks best.
Trying to ‘normalize’a very deficient female chin is usually an aesthetic mistake. It is simply too big of a change from their lifelong reference point. Preoperative computer imaging from at least two different facial angles can help determine how much change will be tolerable.
Case Highlights:
1) Major chin advancements, particularly in females, should be done by a sliding genioplasty to avoid undesirable widening and elongation of the chin.
2) In major female chin advancements the gonion of the chin is angled back and the mental foramen has a high canal position compared to the mental foramen exit. This is why chin implant often don’t work well.
3) Female chin advancements must avoid over correction, particularly in really short chins, where the patient may not recognize themselves with a so called normalized chin position.
Dr. Barry Eppley
Indianapolis, Indiana