

Background: Cartilage grafting is an essential element of many rhinoplasties. Such cartilage grafts are used for two main purposes, structural support and augmentation. For most structural support needs (e.g., columellar strut, spreader grafts) the septal harvest site is usually adequate which may be supplemented by ear grafts. These graft harvest sites are also adequate for most minor to moderate augmentation needs. But when significant nasal augmentation is needed, only a cartilage rib graft harvest will suffice.
Rib grafts have a long history of use in rhinoplasty particular in augmentation of ethnic noses. When the augmentation needed is that of a near L configuration involving the dorsum and the columellar-tip complex, a single cartilaginous rib can provide 5 or 6X more graft volume than that of the septum. But no piece of rib cartilage is ever completely straight nor can it be trusted to be so when placed. This is evident by noting that the only flat geometry of the ribcage is the sternum and not any of its ribs. Carving the straightest piece of the rib graft harvest is helpful but there is always the risk of what was once straight to not be in the future.
If a rib graft is unusable as a solid construct the well known strategy is then to change its structure to that of a diced graft. This approach captures the benefits of its volume and completely eliminates any risk of postoperative shape change. But a diced graft will to work for the tip part of the augmentation where more formed pieces are needed.
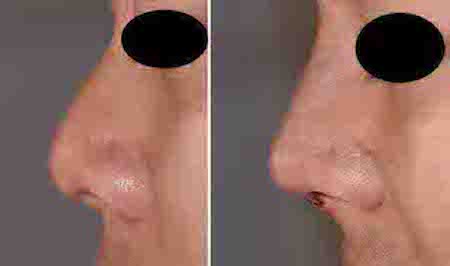
Case Study: This young male wanted to change his nasal shape from that of a ore juvenile nose with a low dorsum and soft rounded tip with a short columella into a more masculine shape. Only a rib graft could provide that much volume.

 Under general anesthesia the cartilaginous portion of rib #8 as harvested. A straighter section was used to carve a solid dorsal onlay graft of 3 to mms thick which was placed into a narrow tunnel on top the middle vault and nasal bones. This was supplemented with a columellar strut, a columellar onlay graft and three layers of shield grafts over the tip. Columellar skin closure was right but the tip skin maintained capillary refill.
Under general anesthesia the cartilaginous portion of rib #8 as harvested. A straighter section was used to carve a solid dorsal onlay graft of 3 to mms thick which was placed into a narrow tunnel on top the middle vault and nasal bones. This was supplemented with a columellar strut, a columellar onlay graft and three layers of shield grafts over the tip. Columellar skin closure was right but the tip skin maintained capillary refill.
 Interestingly there is always the concern of the subcostal scar from the rib graft harvest. But in his case the incision was placed inside an existing tattoo which also allowed a long incisional length than normally would be used.
Interestingly there is always the concern of the subcostal scar from the rib graft harvest. But in his case the incision was placed inside an existing tattoo which also allowed a long incisional length than normally would be used.
Case Highlights:
1) The use of a rib graft in augmentative rhinoplasty is for the purpose of not being ‘graft restricted’, not because it offers the straightest graft shape.
2) Carved solid rib grafts are used for dorsal augmentation and always have the risk of warping. Using sliced pieces for the tip, columella and ala do not usually pose such warping issues.
3) The use of rib grafts presents the uncommon circumstance of creating such tip projection that columellar incisional closure and vascularity of the tip skin may be compromised.
Dr. Barry Eppley
Indianapolis, Indiana