

Background: The scalp is prone to a variety of aesthetic abnormalities which are often not well known or even recognized. One of the more common aesthetic scalp abnormalities are redundant rolls of scalp that typically appear on the back of the head where the scalp meets the neck skin. There is an association of the location of the bottom of the occipital bone and the location of the scalp rolls.With a normal skull shape excess scalp stops at the bottom of the occipital bone, which serves as a soft tissue stop, and where rolls accumulate.
If there is an abnormal skull shape/growth the concept of the scalp stop for roll creation is accentuated as a physical barrier exists. This is seen in some occipital knobs which are central occipital blocks. It is more pronounced when a prominent nuchal ridge exists. This is a which broader line of raised bone and thus it catches more redundant scalp and the scalp roll becomes longer with a deeper horizontal indentation. This may also result in more than one scalp roll known as the double scalp roll. Very rarely a triple scalp roll may even be seen.
The definite treatment for scalp rolls is a horizontally oriented excision. The entire roll or rolls must be incorporated into the excisional pattern for an effective flattening of the back of the head. When an occipital knob or raised nuchal ridge line of bone exists it must be concurrently removed through a bone burring technique. Such bony abnormalities are usually known beforehand by exam and can be palpated at the bottom of the longest scalp roll and deepest line of indentation beneath.
Another factor that must be considered in scalp roll removals is the patient’s natural scalp laxity. If significant scalp laxity exists the amount of horizontal excision needs to be greater than just the scalp roll(s) if a smooth contour is to be achieved. One such condition that is an indicator of significant scalp laxity is CVG or cutis vertices gyrata. While there are linear indentations that run across the scalp of variable depths in CVG the scalp usually is quite mobile/flexible particularly in medium and dark skin pigmented patients.
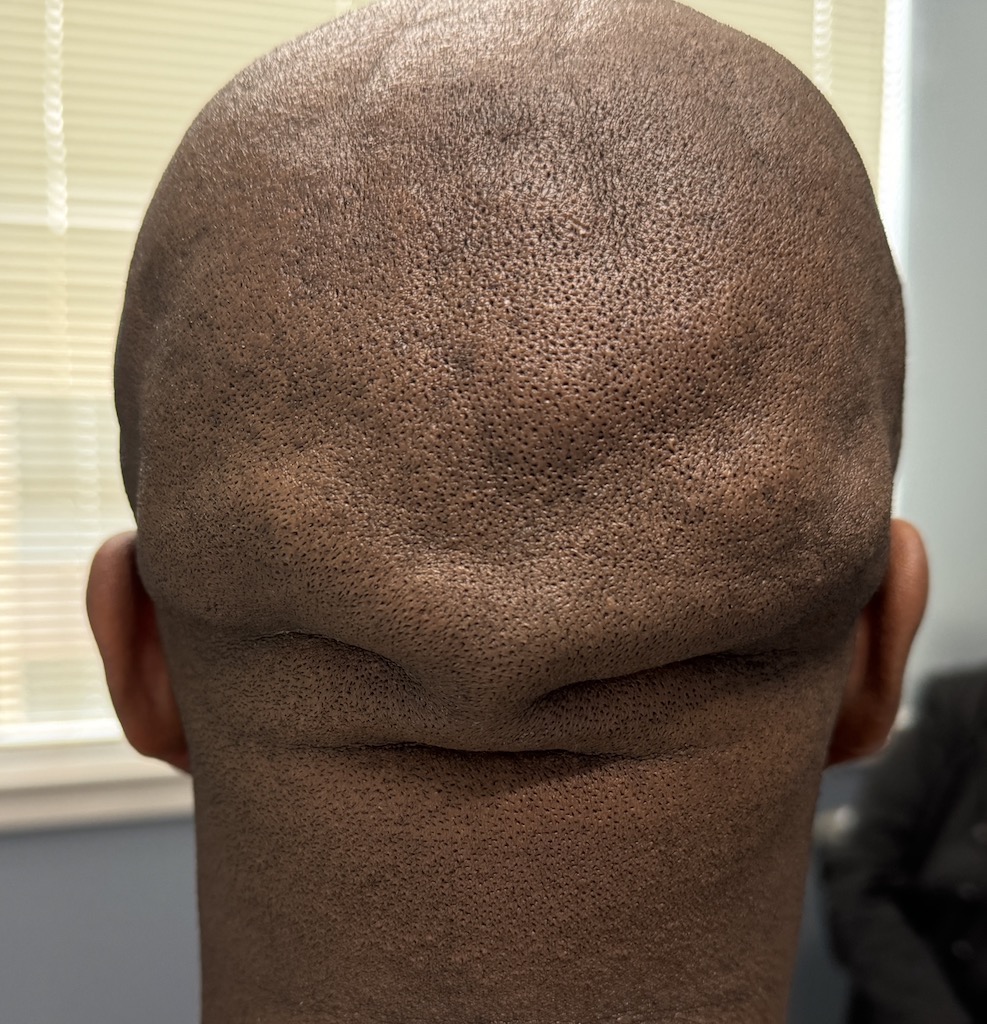
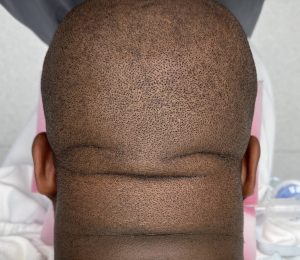
 Case Study: This male presented with double scalp rolls on the back of his head. The larger scalp roll had a distinct gull or eagle wing shape indicative of an enlarged bony nuchal ridge line beneath it. A deep horizontal indentation existed under the large scalp roll which was fixed to the bone.
Case Study: This male presented with double scalp rolls on the back of his head. The larger scalp roll had a distinct gull or eagle wing shape indicative of an enlarged bony nuchal ridge line beneath it. A deep horizontal indentation existed under the large scalp roll which was fixed to the bone.
 Under general anesthesia and in the prone position the scalp rolls were less obvious as the very flexible scalp shifts forward. But when pushed down the scalp rolls become more apparent and even exaggerated due to the extreme scalp laxity. Fine linear lines were seen in the scalp indicative of CVG.
Under general anesthesia and in the prone position the scalp rolls were less obvious as the very flexible scalp shifts forward. But when pushed down the scalp rolls become more apparent and even exaggerated due to the extreme scalp laxity. Fine linear lines were seen in the scalp indicative of CVG.

 Excision of the scalp rolls was done down to fascia with exposure of the bone centrally. The fascia was preserved laterally to avoid injury to the greater occipital neurovascular bundles. The enlarged nuchal ridge was reduced by cutting it off with a reciprocating saw.
Excision of the scalp rolls was done down to fascia with exposure of the bone centrally. The fascia was preserved laterally to avoid injury to the greater occipital neurovascular bundles. The enlarged nuchal ridge was reduced by cutting it off with a reciprocating saw.

 A multi-layer closure with done quilting the deeper tissues down to the fascia so a drain was not needed. The incision line represented the now transition between the loose CVG scalp skin and the smoother neck skin. The scalp closure was then heavily taped for a dressing.
A multi-layer closure with done quilting the deeper tissues down to the fascia so a drain was not needed. The incision line represented the now transition between the loose CVG scalp skin and the smoother neck skin. The scalp closure was then heavily taped for a dressing.

 When seen the next day the improvement in the contour of the back of his head was seen even through the heavy taping that was present.
When seen the next day the improvement in the contour of the back of his head was seen even through the heavy taping that was present.
Scalp rolls associated with enlargements of occipital bone areas present a multifactorial reason for their existence. Such bony involvements can usually be determined preop. While the soft tissue scalp rolls are bigger in surface area than that of the enlarged bone, removal of the bone is still integral to the best contour reduction.
Key Points:
1) Many scalp rolls are associated and partially caused by a prominent or overgrown nuchal ridge skull line.
2) The bony scalp roll has a nuchal ridge that catches the scalp and creates a horizontal crease underneath.
3) Scalp rolls are particularly prone to occur in patients with significant scalp laxity which can be associated with CVG.
Dr. Barry Eppley
World-Renowned Plastic Surgeon