


Background: Augmentation by numerous methods is by far the most common aesthetic lip procedure. Going the other way, as in lip reductions, is a much more uncommon lip size change. But there are patients who feel embarrassed by the natural size of their lips and desire them to be reduced.
In addition to its infrequency there is no easy or injectable method of lip reduction. It can only be performed by excision of tissue from the lip itself. It is best thought as a reverse lip advancement where internal tissues are removed and the vermilion-cutaneous edge is rolled inward as a result. The key question is where should the excision be done and, in doing so, how well does it hide the scar.
The tissue that needs to be excised in lip reduction is the dry vermilion. While the wet mucosa behind the wet-dry line is tempting to take because it optimally hides the scar line, it does not make for an effective lip reduction. The wet mucosa is too mobile and all that usually happens is that the back edge of the excision site is pulled forward rather than the vermilion cutaneous junction of the outer lip edge being pulled back. This results in no significant lip reduction. And when a patient tells me that they have had a lip reduction procedure and only very modest improvements are seen, I automatically know where the excision on the lip was done at. (or they took it from the right location but took too little)
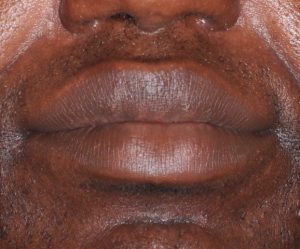
 Case Study: This male had a prior history of lip implants, subnasal lip lift, vermilion advancements and lip reductions. He wanted further lip reduction but wanted to keep the lip implants inlace to maintain forward projection/pout.
Case Study: This male had a prior history of lip implants, subnasal lip lift, vermilion advancements and lip reductions. He wanted further lip reduction but wanted to keep the lip implants inlace to maintain forward projection/pout.
 Under general anesthesia the markings for the lip reduction were done. The back edge was the previous scar and the front edge was out on the dry vermilion.
Under general anesthesia the markings for the lip reduction were done. The back edge was the previous scar and the front edge was out on the dry vermilion.
 The elliptical excisions were done inside each mouth corner using a scalpel for the initial incision lines and needle point cautery for the scar/vermilion excision. The lip implants were not encountered.
The elliptical excisions were done inside each mouth corner using a scalpel for the initial incision lines and needle point cautery for the scar/vermilion excision. The lip implants were not encountered.
 A double layer closure was done using 5-0 vicryl deep and running 5-0 chromic for the vermilion-mucosal closure.
A double layer closure was done using 5-0 vicryl deep and running 5-0 chromic for the vermilion-mucosal closure.
The two key points are that the dry vermilion must be the tissue removed and a deeper wedge excision is not done/needed. (this avoids a lot of bleeding, swelling and protracted numbness.
Case Highlights:
1) Lip reduction are frequently done by removing the wet mobile mucosa behind the wet-dry line…which will produce minimal to no external lip reduction.
2) Visible lip reduction requires removal of the dry vermilion with the back incision at the wet-dry line.
3) Lip reductions can be done with indwelling lip implants without exposing them.
Dr. Barry Eppley
Indianapolis, Indiana