

Background: The appearance/size of the brow bones is a forehead feature that is usually very gender specific. Prominent brow bones is a verydistinct male trait and serves as the basis for why forehead reshaping is one of the most common facial feminization surgery procedures. Often lost in this surgery is that brow bone reductions are also done in men with the same surgical techniques. The differences between transfemale and cis-male brow bone reductions are the size of the treated brow bones (males seek reduction of much larger brow bone protrusions) and the consideration of incisional access and the resultant scar.
There are two basic techniques in brow bone reductions which differ in the management of the protrusive outer table of the frontal sinus. The outer table can be reduced in place (burring) or in can be removed and reshaped/repositioned. (bone flap setback) These two methods can have very different aesthetic outcomes as the thickness of the outer table of bone is not thick (usually 4mms or less) which makes burring a less effective reduction technique that decreasing the size of the frontal sinus air space. (bone flap setback)
While the bone flap setback technique is going to be the most effective brow bone reduction technique for most men, the incisional access to do it may be a limiting factor due to the patient’s hairline/hair density. Thus a burring technique may be initially attempted through less of a scalp incision, hoping this more limited reduction would be adequate. If it is not aesthetically satisfactory can a bone flap reduction then be done secondarily?
Case Study: This young male desired a brow bone reduction procedure that produced a significant flattening but scar limitation was an initial goal. Through a retro hairline incision a bone burring technique was done which was beneficial but not as much as he had hoped. He was now ready to accept a longer scalp incision to enable a bone flap setback procedure to be done.

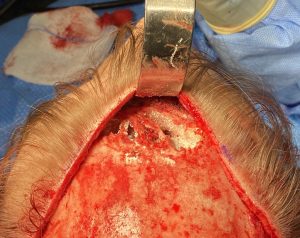
 Under general anesthesia and through a longer scalp incision that extended into the upper temporal area the forehead flap was turned down to expose the previously reduced brow bones. The amount of prior reduction could be appreciated by the very thin layer of remaining outer table bone and even a few small perforations.
Under general anesthesia and through a longer scalp incision that extended into the upper temporal area the forehead flap was turned down to expose the previously reduced brow bones. The amount of prior reduction could be appreciated by the very thin layer of remaining outer table bone and even a few small perforations.

 Using a long reciprocating saw blade the remaining outer table of bone was removed. It was very thin and ended up fracturing into several segments. A high speed handpiece and burr was then used to reduce the surrounding perimeter of bone around the frontal sinus with emphasis on the lower ridge of bone along the inferior orbital rim and across the nose.
Using a long reciprocating saw blade the remaining outer table of bone was removed. It was very thin and ended up fracturing into several segments. A high speed handpiece and burr was then used to reduce the surrounding perimeter of bone around the frontal sinus with emphasis on the lower ridge of bone along the inferior orbital rim and across the nose.
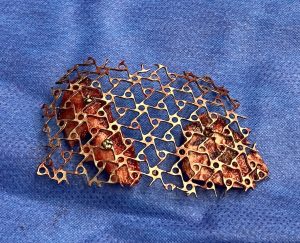
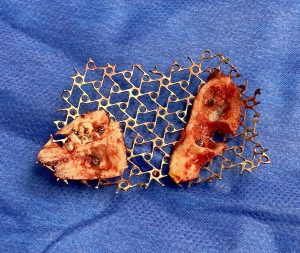 To reassemble the bone fragments into a stable construct to be set back a 1mm titanium mesh was used.The bone was fixed to the mesh at various locations with the largest underlying bone defects.
To reassemble the bone fragments into a stable construct to be set back a 1mm titanium mesh was used.The bone was fixed to the mesh at various locations with the largest underlying bone defects.
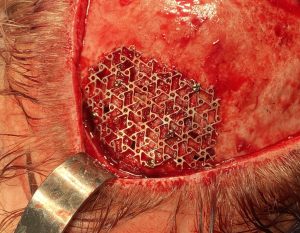
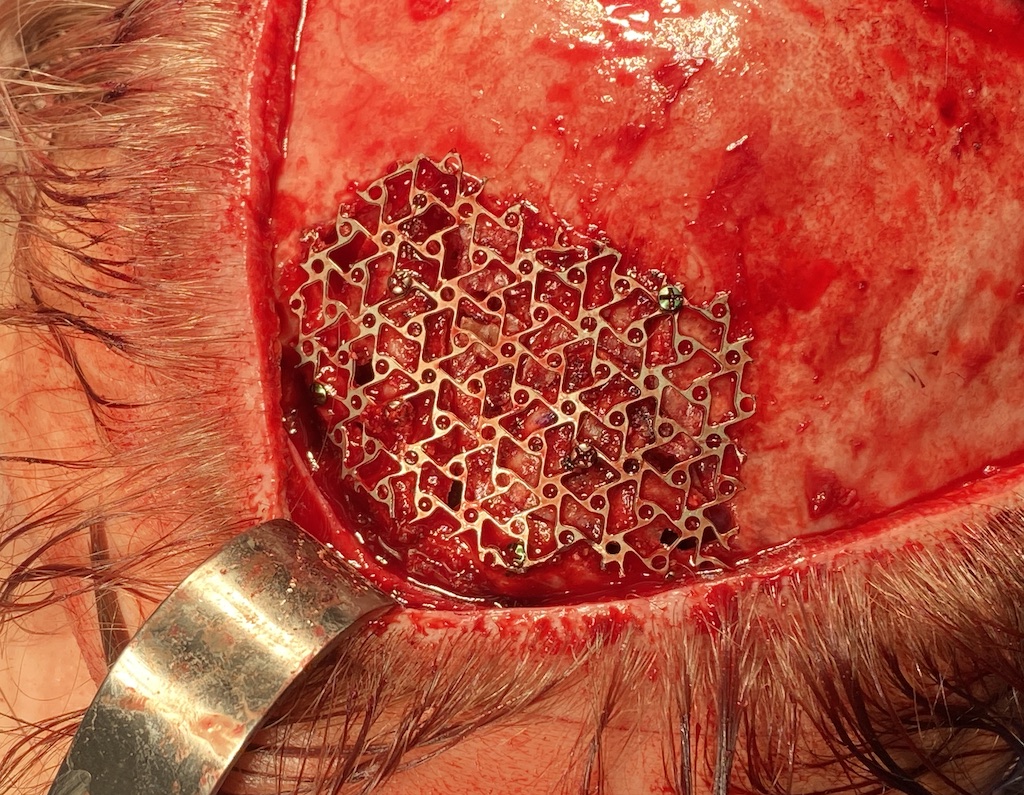
 The mesh-bone construct was then put back over the open frontal sinus and tacked around its edges with 1mm microscrews.
The mesh-bone construct was then put back over the open frontal sinus and tacked around its edges with 1mm microscrews.

 The forehead flap was put back and closed with a two layer resorbable suture closure over a drain. A secondary rhinoplasty was then performed. His immediate before and after profile showed the secondary brow bone reduction achieved.
The forehead flap was put back and closed with a two layer resorbable suture closure over a drain. A secondary rhinoplasty was then performed. His immediate before and after profile showed the secondary brow bone reduction achieved.

 In comparing the initial before surgery profile with the 2nd stage brow bone reduction the even greater change could be appreciated.
In comparing the initial before surgery profile with the 2nd stage brow bone reduction the even greater change could be appreciated.
The goal of brow bone reduction surgery is to get an effective result in one surgery. And this is almost always accomplished with the bone flap setback technique. But this technique requires adequate access which usually requires a longer scalp incision. In men this is often a challenge given the hair differences between most men and women. Burring reduction can usually be performed with a more limited scalp incision but with the understanding that the amount of setback will be less.
In this case this was initially done and, although some good improvement was obtained, the patient desired more. With a longer incision a secondary bone flap removal was successfully done which necessitated an uncommon mesh screen method of creating a stable construct over the fontal sinus to hold the removed bone fragments. This combo all-plastic-autologous anterior table of the frontal sinus allowed for an effective brow setback to the completed.
Case Highlights:
1) Of the two forms of brow bone reduction the bone flap setback technique produces a more significant effect.
2) When doing secondary brow bone reduction by bone flap setback after an initial burring management of the thin and friable bone flap and setting it back will be more challenging.
3) A micromesh screen for fixing the fragmented thin bone flap is an effective secondary bone fixation method over the open frontal sinus cavity.
Dr. Barry Eppley
World-Renowned Plastic Surgeon