

Background: The occipital bone is a large skull bone of which most is not seen as it lies below the neck muscles and wraps inferiorly around the spine. The part that is seen is the upper portion of the occipital bone which is prone to various protrusions such as knobs and buns. But in the scaphocephalic head shape, often due to untreated or inadequately treated sagittal craniosynostosis, the entire visible occipital bone will be protrusive as the head is elongated both anteriorly and posteriorly.
In the adult scaphocephalic head shape correction, which always involves a custom skull implant, but often will need some occipital bone reduction as well. Since the scaphocephalic procedure is done from a more superior incisional location the back is reduced from the top down. While this does provide some very effective reduction it is difficult to get at and below the thick nuchal ridge. As a result complete reduction of the protruding occipital bone may not be fully achieved.

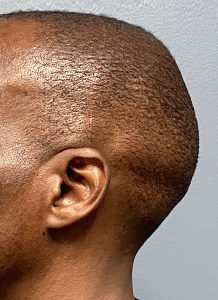 Case Study: This male had a prior extensive skull reshaping procedure done through a full bicoronal scalp incision for his scaphocephalic head shape. This consisted of the placement of large skull implant as well as frontal and occipital bone reduction. An extensive occipital bone reduction was done from this superior approach. While this provided very good improvement he desired secondary occipital reduction if possible.
Case Study: This male had a prior extensive skull reshaping procedure done through a full bicoronal scalp incision for his scaphocephalic head shape. This consisted of the placement of large skull implant as well as frontal and occipital bone reduction. An extensive occipital bone reduction was done from this superior approach. While this provided very good improvement he desired secondary occipital reduction if possible.

 Under general anesthesia and in the prone position a small incision was made directly over nuchal ridge. Through this incision the nuchal ridge bone was reduced as much as possible by high speed burring. Closure was done over a drain in multiple layers with resorbable sutures.
Under general anesthesia and in the prone position a small incision was made directly over nuchal ridge. Through this incision the nuchal ridge bone was reduced as much as possible by high speed burring. Closure was done over a drain in multiple layers with resorbable sutures.
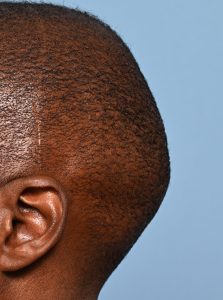
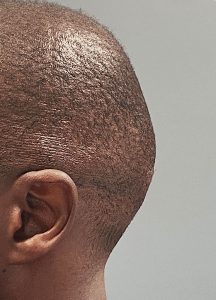 When seen the next day for drain removal the secondary improvement in the low residual occipital projection could be seen.
When seen the next day for drain removal the secondary improvement in the low residual occipital projection could be seen.
 This small scalp incision should heal in an inconspicuous fashion, better than his coronal scalp incision.
This small scalp incision should heal in an inconspicuous fashion, better than his coronal scalp incision.
Getting maximal reduction of an overall occipital protrusion can be difficult from any one single incisional approach. While the coronal scalp incision provides great access to many parts of the skull it is difficult to get low down over the nuchal ridge. Conversely a low scalp incision over the nuchal ridge has difficulty getting to the most superior aspect of the occipital protrusion. In this
Key Points:
1) A superior occipital reduction has difficulty adequately reducing the full extent of the nuchal ridge protrusion.
2) A direct incision over the nuchal ridge allows for optimal reduction of the lowest portion of the visible occipital bone.
3) The maximal reduction of the entire occipital bone may require a dual incisional approach.
Dr. Barry Eppley
World-Renowned Plastic Surgeon