

Background: The skull is prone to numerous contour deformations for which augmentation materials can be used to improve its shape. Plagiocephaly is the most recognized of all the deformational skull shape concerns. While it does affect the entire skull by far the most severely affected area is the back of the head one side being flattened. For whatever reason plagiocephaly in my experience affects the right back side of the head most frequently.
Plagiocephaly can largely be corrected by placement of an implant on top of the flattened deformed bone. By history the use of bone cements was the only method for skull augmentation and the options were acrylic (PMMA)and hydroxyapatite (HA) cement. When they were the only augmentation options available they seemed reasonable to use. However with the emergence of 3-D CT scanning and custom implant designs they have largely been relegated to a much more limited role in skull augmentations. What 3-D CT scanning has shown is that the surface area involvement in any skull contour issue is far greater than what can be appreciated by any external visual assessment. In addition pushing small amounts of bone cement through small scalp incisions, to no surprise, produces a very inadequate skull contour restoration.
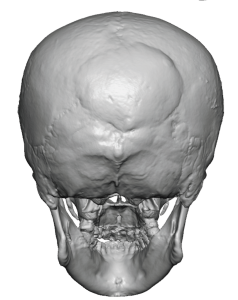
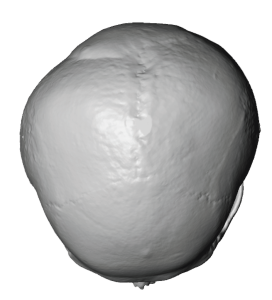 Case Study: This male had a plagiocephalic skull deformity with a flattened right back of the head. It was treated 10 years ago with the placement of hydroxyapatite cement. The patient always felt that this provided an inadequate correction very limited benefit. His 3-D CT skull scan showed the presence of a right flat back of the head with a central location of a mound of hydroxyapatite cement.
Case Study: This male had a plagiocephalic skull deformity with a flattened right back of the head. It was treated 10 years ago with the placement of hydroxyapatite cement. The patient always felt that this provided an inadequate correction very limited benefit. His 3-D CT skull scan showed the presence of a right flat back of the head with a central location of a mound of hydroxyapatite cement.
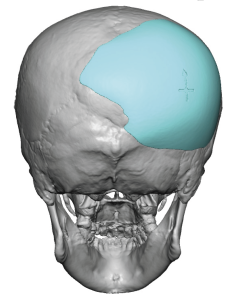
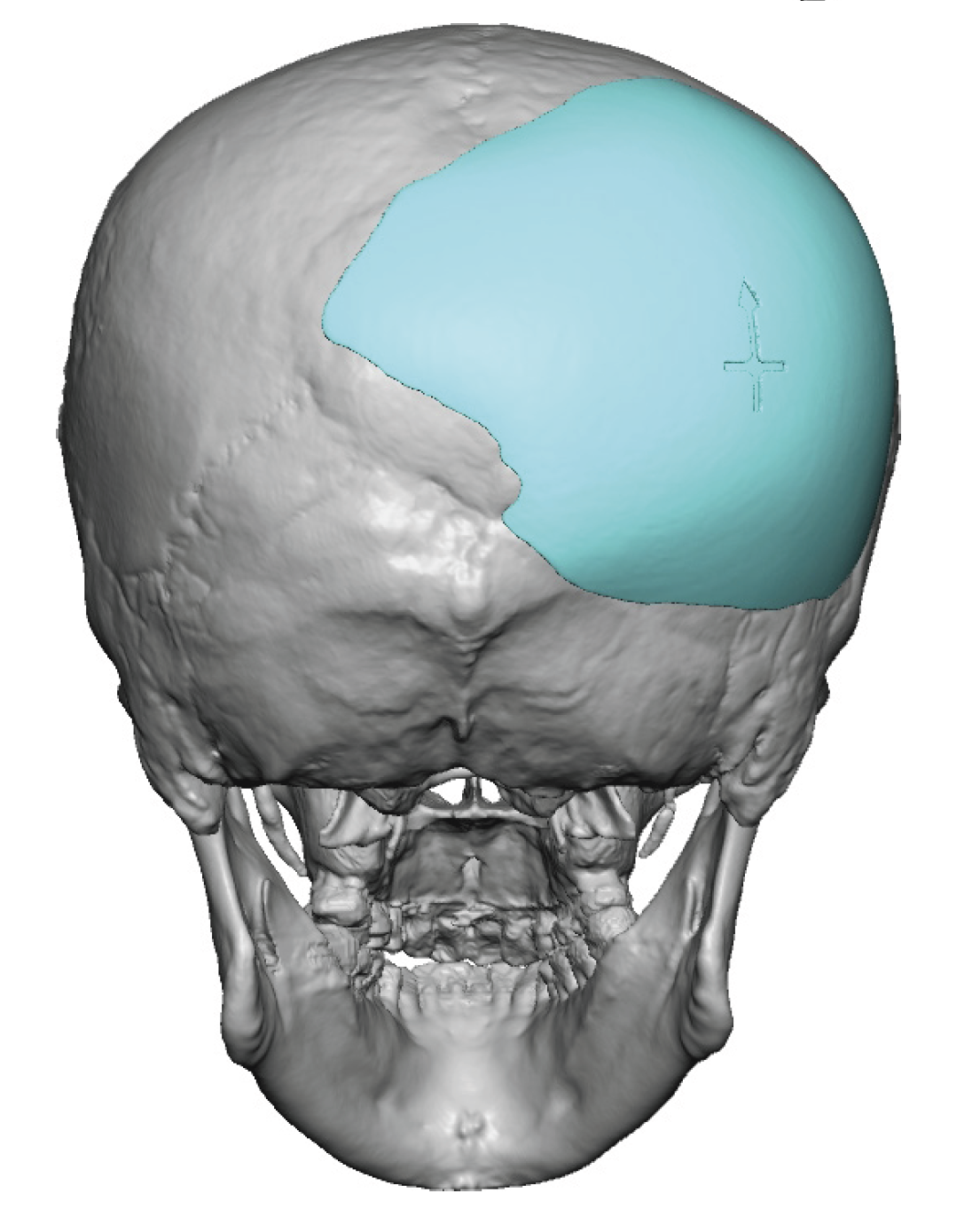
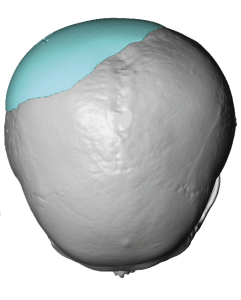 A custom skull implant was designed to provide a more complete correction of the right flat back of his head. Its design encompassed part of the hydroxyapatite cement going around and over it.
A custom skull implant was designed to provide a more complete correction of the right flat back of his head. Its design encompassed part of the hydroxyapatite cement going around and over it.
 Under general anesthesia and in the prone position a small scalp incision was made over the lower end of the hydroxyapatite cement. The cement could clearly be differentiated from the surrounding bone by its very white color. The hydroxyapatite cement was firmly attached to the underlying bone.
Under general anesthesia and in the prone position a small scalp incision was made over the lower end of the hydroxyapatite cement. The cement could clearly be differentiated from the surrounding bone by its very white color. The hydroxyapatite cement was firmly attached to the underlying bone.
 The custom skull implant was prepared for placement by creating multiple 4 mm perfusion holes with a dermal punch.
The custom skull implant was prepared for placement by creating multiple 4 mm perfusion holes with a dermal punch.
 The implant was inserted through the small scalp incision and then positioned per the implant design. Proper positioning of the implant was aided by how it wrapped around part of the hydroxyapatite cement. It was then secured with a single microscrew. The incision was then closed over a drain.
The implant was inserted through the small scalp incision and then positioned per the implant design. Proper positioning of the implant was aided by how it wrapped around part of the hydroxyapatite cement. It was then secured with a single microscrew. The incision was then closed over a drain.

 The immediate effects and improvement of the right back of the head contour could be seen immediately at the conclusion of the surgery.
The immediate effects and improvement of the right back of the head contour could be seen immediately at the conclusion of the surgery.
Hydroxyapatite cement is the most biocompatible implant that can be used for the skull. But despite its biologic advantages it has numerous disadvantages which make it an inferior skull augmentation material. Lack of visualization of its placement and control of its shape as it sets when using small scalp incisions limits its effectiveness. There is also the disadvantage of a soft putty like material trying to significantly push out a tight scalp area. All of these placement characteristics relegates hydroxyapatite cement to a very limited role i n anesthetic skull augmentation.
But since this cement bonds directly to the skull it does not need to be removed later for secondary skull augmentation. It can be maintained in place and a custom implant can be place over and around it without concerns about disruption or fracture of the cement. So in some ways the initial use of hydroxyapatite cement was not completely useless and does provide a platform to guide further skull augmentation in the future.
Highlights:
- The use of hydroxyapatite cement for plagiocephaly surgery for back of the head augmentation produces an inadequate correction.
- A custom back of the head skull implant provides the best plagiocephaly correction and indwelling hydroxyapatite cement can be maintained with an implant design over and around it.
- The placement of a custom back of the head skull implant can be done through a remarkably small scalp incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon