

Background: The use of an implant to correct a small chin is one of the most common facial reshaping procedures. Conceptually it is a very straightforward procedure but consistently getting good aesthetic results is dependent on numerous variables such as implant style and size, its position on the bone and ultimately the patient’s response to its aesthetic effects.
When patient’s are unhappy with their primary chin augmentation results, and the culprit is lack of adequate forward projection, the patient has two options. A new larger chin implant can be placed or a completely different approach of a sliding genioplasty can be used. That choice is influenced by how much further chin augmentation is needed, how much was originally achieved and whether there were any problems or concerns with the initial implant. (e.g., asymmetry, nerve symptoms) For example, if only a few more millimeters are needed then it would make the most sense to simply switch to a bigger implant. But if the amount needed is more substantial there may be reasons to change to a sliding genioplasty.
When converting from a chin implant to a sliding genioplasty the question is always what dimensional changes are needed. External measurements and computer imaging are most useful to do so. When measuring externally one needs to add the existing chin implant thickness, if known, onto the additional amount needed. If not known it will be quickly determined during surgery.
Case Study: This female had a prior chin implant which she felt right after surgery was inadequate in forward projection and length. She also did not like how wide it made her chin. The exact dimensions of the chin implant were unknown. Computer imaging and measurements showed that an additional 5mms of horizontal projection was desired along with 3mms of vertical lengthening.

 Under general anesthesia and through an intraoral approach, the chin implant was exposed and removed. It was a 5mm mandibular glove style silicone implant. Its width that it adds to the female chin can be seen.
Under general anesthesia and through an intraoral approach, the chin implant was exposed and removed. It was a 5mm mandibular glove style silicone implant. Its width that it adds to the female chin can be seen.

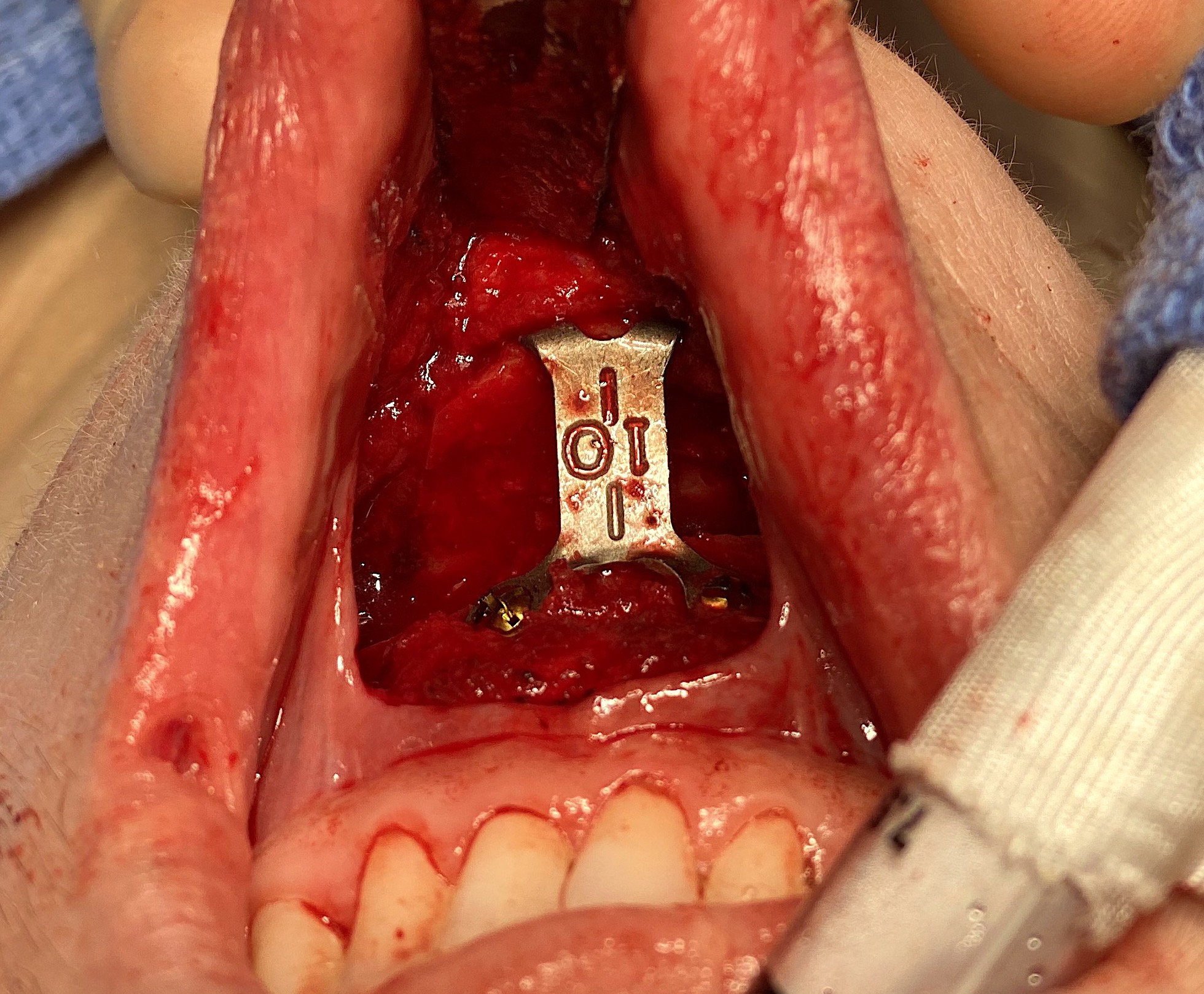
 The implant capsule was removed from the bone. Because the chin implant was symmetrically placed and in a low position on the bone, the full-thickness bone cut was made along the superior edge of the implant capsule from side to side. The bone was advanced 10mms using a step plate. The step plate was bent down to get the 3mm vertical lengthening. With a large bony step off and opening caused by the large advancement, tissue bank bone chips was grafted into this induced bony ‘defect’.
The implant capsule was removed from the bone. Because the chin implant was symmetrically placed and in a low position on the bone, the full-thickness bone cut was made along the superior edge of the implant capsule from side to side. The bone was advanced 10mms using a step plate. The step plate was bent down to get the 3mm vertical lengthening. With a large bony step off and opening caused by the large advancement, tissue bank bone chips was grafted into this induced bony ‘defect’.
When a chin implant is being converted into a sliding genioplasty, much of the tissue dissection/release may already have been done by the implant pocket….provided the implant is the proper position and has an extended wing style.
Case Highlights:
1) A chin implant can be a prelude to another effort at chin augmentation if it is dimensionally inadequate. (e.g., not enough projection)
2) When the chin implant is removed the superior border of the implant pocket provides the cut line for a sliding genioplasty…provided the chin implant was an extended style and was positioned low enough on the bone.
3) The projection of the indwelling chin implant combined with external measurements provides the amount of horizontal movement is needed in the new sliding genioplasty.
Dr. Barry Eppley
Indianapolis, Indiana