

Background: The sliding genioplasty is a versatile chin reshaping procedure that has as its main advantage being an autologous procedure. Cutting and moving one’s chin bone has a very low rate of infection (I have only seen one) and assured healing every time. (in my experience) Despite its more invasive nature it is a safe and effective procedure as long as it can meet the patient’s aesthetic chin needs.
One of its disadvantages over a chin implant, however, is that it is not as easily revised or reversed. To repeat the intraoral osteotomy requires a bigger commitment on the patient’s part that exchanging a chin implant does. From a technical and healing standpoint pertinent questions include is it harder to do than the first time, will the bone heal as well and are there increased risks by cutting the bone twice?
Almost regardless of the direction that the chin bone is moved (most commonly moved forward) the original osteotomy is visible and is used to repeat the bone cut. With forward movements in particular the actual thickness of the bone is usually less and often is more easily cut. Since it is the original osteotomy line the mental nerve should not be affected if it was not the first time.
Case Study: This male had a sliding genioplasty of 8mm one year previously. He initially went conservative with the advancement as he did not want to go too big. But as he got accustomed to the new chin he eventually decided that he wanted some additional horizontal chin projection.

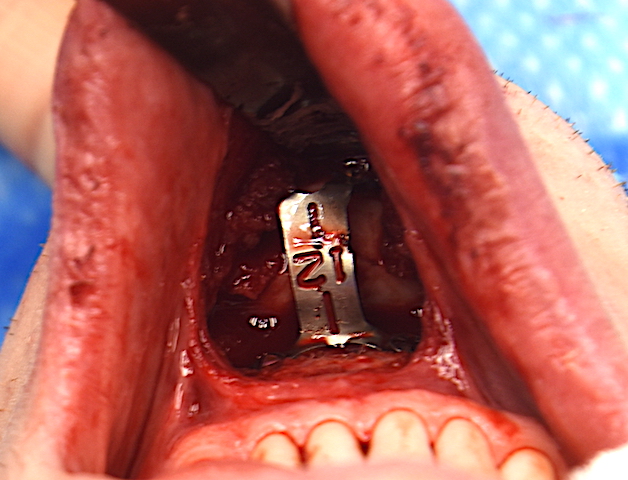
 Under general anesthesia on the inside of the lower lip his original intraoral vestibular incision showed a well healed incision with minimal scarring. This was reopened and the chin plate/osteotomy site exposed. A very thin of bone had overgrown on the upper part of the plate.
Under general anesthesia on the inside of the lower lip his original intraoral vestibular incision showed a well healed incision with minimal scarring. This was reopened and the chin plate/osteotomy site exposed. A very thin of bone had overgrown on the upper part of the plate.

 The plate and screws were easily removed and the bone was well healed albeit with a step shape to it. The original osteotomy line was not discernible but they step shape of the bone provided the location of it. It was recut with good solid bone throughout and then downfractured.
The plate and screws were easily removed and the bone was well healed albeit with a step shape to it. The original osteotomy line was not discernible but they step shape of the bone provided the location of it. It was recut with good solid bone throughout and then downfractured.
 It was advanced out to 12mms with a new plate using the original screw holes. The enlarged stem deformity of the bone was grafted with 5ccs of tissue back corticocancellous bone chips and then closed.
It was advanced out to 12mms with a new plate using the original screw holes. The enlarged stem deformity of the bone was grafted with 5ccs of tissue back corticocancellous bone chips and then closed.

 Taking him back to his first sliding genioplasty procedure he finally achieved his optimal chin augmentation result.
Taking him back to his first sliding genioplasty procedure he finally achieved his optimal chin augmentation result.
Estimating how much forward projection is desired in a sliding genioplasty will vary based on the patient’s goals and gender. Patients understandably fear doing too much and this is of particular relevance in women. Men often prefer to go on the stronger side of change and usually undergo larger amounts of bone advancement. But for those men that didn’t go far enough the first time a secondary sliding genioplasty can be successfully performed with not greater risks than the first time.
Case Highlights:
1) A sliding genioplasty can be successfully performed twice (secondary genioplasty) without any bone healing issues.
2) In secondary genioplasty it is prudent to graft the osteotomy site with allogeneic corticocancellous bone chips.
3) Patients should expect the second sliding genioplasty to be a less traumatic experience than the first time in most cases.
Dr. Barry Eppley
Indianapolis, Indiana