


Background: The width and shape of the shoulders is highly gender specific. While broad shoulders are desired by most men, more narrow shoulders are usually preferred by women. Men prefer a sharper shoulder shape while women a more rounder one. While men seek surgical methods to large their shoulders, women may seek a method to reduce them. Shoulder widening has three methods to do so while shoulder reduction has only one. (clavicle reduction osteotomies)
While the perception of one’s shoulder width is what ultimately matters, there are several methods used to measure or quantitate it. Typically shoulder width is measured from tip to tip which is the acromio-clavicular prominence. A more complicated method is biacromial width which measures the outermost bony points on the top of each shoulder. Another method, which I find the most useful as it contributes the most to the visual perception of the shoulders, is bideltoid width. This will be greater than biacromial width because it includes the soft tissues (muscle and fat) as well.
While women often seek to know what their bideltoid width is and whether it is normal or not, it is not quite that simple. Tables certainly exist for bideltoid widths but there are a lot of factors (height and weight, ethnicity) that go into these measurements and I would not get too restrictive by some table. It is more about proportion and the patient’s perception of it than any number. Bideltoid width is relevant for me because it can be measured before and after shoulder reduction surgery as a measure of effectiveness of the bone removed and the amount of bideltoid reduction that occurs from it.
 Case Study: This female presented for shoulder width reduction. She was tall and thin and felt her shoulders were too wide. Her bideltoid width was 48cms. Clavicle length was 16cms.
Case Study: This female presented for shoulder width reduction. She was tall and thin and felt her shoulders were too wide. Her bideltoid width was 48cms. Clavicle length was 16cms.


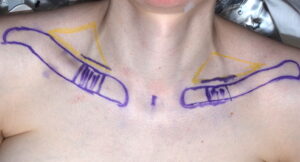
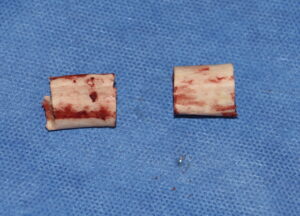
 Under general anesthesia an incision was made in the supraclavicular fossa to access the medial third of the clavicles. With circumferential isolation of the bone a 3cm segment was removed.
Under general anesthesia an incision was made in the supraclavicular fossa to access the medial third of the clavicles. With circumferential isolation of the bone a 3cm segment was removed.

 The shoulders were brought in and the clavicle ends aligned and held together with a superior plate and screws. An anterior plate and screws were then applied for additional fixation security.
The shoulders were brought in and the clavicle ends aligned and held together with a superior plate and screws. An anterior plate and screws were then applied for additional fixation security.
 Closure was done by repositioning muscle back up over the plates followed by fascia/fat and skin closure.
Closure was done by repositioning muscle back up over the plates followed by fascia/fat and skin closure.
 While the amount of clavicle bone removal has its limitations in shoulder narrowing surgery, the height of the patient and clavicle bone length must be taken into consideration. While generally 2.0 to 2.5cms is taken per side, the longer the natural clavicle is the more that can be taken. As long as the ratio remains under 20% there is no risk of causing any adverse postoperative shoulder function.
While the amount of clavicle bone removal has its limitations in shoulder narrowing surgery, the height of the patient and clavicle bone length must be taken into consideration. While generally 2.0 to 2.5cms is taken per side, the longer the natural clavicle is the more that can be taken. As long as the ratio remains under 20% there is no risk of causing any adverse postoperative shoulder function.
 Shoulder width reduction does make the shoulders more narrow by a reduction in bideltoid measurements. But I would not consider that effect a dramatic one. I think what makes it effective is in the appearance of the reduced angularity/sharpness of the shoulders which is improved by the inward and slightly forward movement of the widest part of the shoulders. This is the result not a geometric effect of the fact that the clavicle is not a completely horizontal bone. Its curved shape
Shoulder width reduction does make the shoulders more narrow by a reduction in bideltoid measurements. But I would not consider that effect a dramatic one. I think what makes it effective is in the appearance of the reduced angularity/sharpness of the shoulders which is improved by the inward and slightly forward movement of the widest part of the shoulders. This is the result not a geometric effect of the fact that the clavicle is not a completely horizontal bone. Its curved shape
Case Highlights:
1) Broad shoulders can be measured by several methods but the patient’s perception of their width is what matters the most.
2) In the taller patient greater bone removal (3cms) of the clavicles can be done as their clavicle lengths and bideltoid widths are greater.
3) Double plate fixation of clavicle reduction osteotomies provides greater assurance against postoperative complications and potentially earlier arm range of motion.
Dr. Barry Eppley
Indianapolis, Indiana