


Background: For the female that is bothered by disproportionately wide shoulders this width can be successfully reduced by clavicle reduction osteotomies. Since the clavicle is the only horizontally oriented bone in the body whose main purpose is to keep the shoulders widely separated from the sternum, reducing its length is the only method by which the width of the shoulders could be reduced.
A unique element of aesthetic shoulder narrowing surgery is its bilateral need and usual performance. While it is entirely possible to undergo one shoulder reduction at a time, the need for two separate surgeries spaced three to six months apart poses its own logistical issues. When done together the recovery issues are not really pain but the need for limited use of both arms. While plate and screw fixation is used one still need to be cautious as good bony alignment in a highly loaded bone does not always guarantee that uncomplicated bony healing will occur.
The accepted technique for clavicle reduction osteotomies is a single 2.7mm plate placed on the bone’s superior surface with three bicortical screws per side. Patients are placed on a limited to progressive arm range of motion protocol for six weeks after the surgery. This approach has been shown to be successful with a very low fixation failure rate (2%) in my experience. But the recovery can be challenging based on the support system which surrounds the patient. This raises the question of whether a more advanced form of clavicle plate fixation may allow for an earlier arm range of motion recovery.

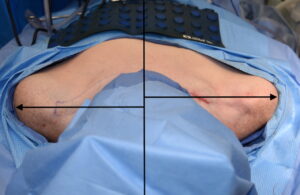
 Case Study: This female was bothered by the width of her shoulders which had a 49cm bideltoid distance. Preoperative shoulder width reduction markings were made with 3.5cm long incision in the supraclavicular fossa.
Case Study: This female was bothered by the width of her shoulders which had a 49cm bideltoid distance. Preoperative shoulder width reduction markings were made with 3.5cm long incision in the supraclavicular fossa.

 On the right side through the supraclavicular skin incision a 3cm segment of medial clavicle bone was removed.
On the right side through the supraclavicular skin incision a 3cm segment of medial clavicle bone was removed.

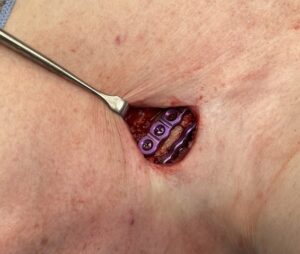
 When the bone segment is removed the shoulder automatically collapses inward shortening the inter bony gap. The bone segments were aligned and secured with a superior 2.7mm seven hole plate with six screws and an anterior five hole plate with four bicortical screws.
When the bone segment is removed the shoulder automatically collapses inward shortening the inter bony gap. The bone segments were aligned and secured with a superior 2.7mm seven hole plate with six screws and an anterior five hole plate with four bicortical screws.
 In comparing the reduced right side with the unreduced left side the more inward and anteriorly positioned right shoulder could be seen.
In comparing the reduced right side with the unreduced left side the more inward and anteriorly positioned right shoulder could be seen.

 On the left side a similar 3cm medial segment of clavicle bone was removed with the identical double plate and screw fixation.
On the left side a similar 3cm medial segment of clavicle bone was removed with the identical double plate and screw fixation.
While she started out with the typical limited arm range of motion, by three weeks after surgery she had non-load bearing arm range of motion up to 90 degrees. This would be weeks ahead of where I would allow a patient with single plate and screw fixation.
The clavicle is an S-shaped long bone whose biomechanics behavior is different from that of a similarly tubular but straight bone. Because of its shape a compressive load placed along its axis results in the greatest stress at the curved middle portion of the bone…which is where most clavicle fractures occur. Medial clavicle osteotomy fixation is inherently more stable than mid-shaft clavicle fracture repair because the compressive loading is supported better by the thicker bone diameter and the greater stability by being closer to a stable sternal base. This explains why a single superior plate fixation works successfully in shoulder reduction surgery whereas a much higher rate of failure would occur if a similar fixation technique was used in mid-shaft clavicle fractures.
The use of double plate clavicle fixation allows for an earlier use of the arms in terms of range of motion. As a result this also makes it less onerous on the patient to perform shoulder width reduction surgery on both sides at the same time.
Case Highlights:
1) The width of the female shoulders can be successfully reduced by an inch per side through removal of a segment of the clavicle.
2) Rigid plate and screw fixation of the shortened clavicle is required in shoulder reduction surgery for assured bone healing for which no absolute standard technique has been proven best.
3) Double plate fixation of reduced clavicles allows for a more rapid recovery with earlier arm range of motion.
Dr. Barry Eppley
Indianapolis, Indiana