

Background: The skull is prone to deformational forces during its development which can adversely affect its shape. While these effects can occur anywhere on the five surfaces of the skull they are most commonly seen on the back of the head. This is probably due to the neonate’s head’s position in utero and most certainly the infant’s head positioning after birth.
By far the most common back of head shape deformity is plagiocephaly or a one-sided flattening. Less commonly seen is complete flattening of the normal convex shape of the back of the head. (brachycephaly) Brachycephaly presents on the back of the head with a variety of presentations. In its non-syndromic form it appears as a flattening of the occipital bone only, sparing much of the parietal bone flattening that occurs in syndromic forms. It can appear as a central occipital flattening or can even appear as an indentation bordered by the lambdoidal sutures superiorly. In side view the back of the head looks cut off or that the most posterior projection is missing.
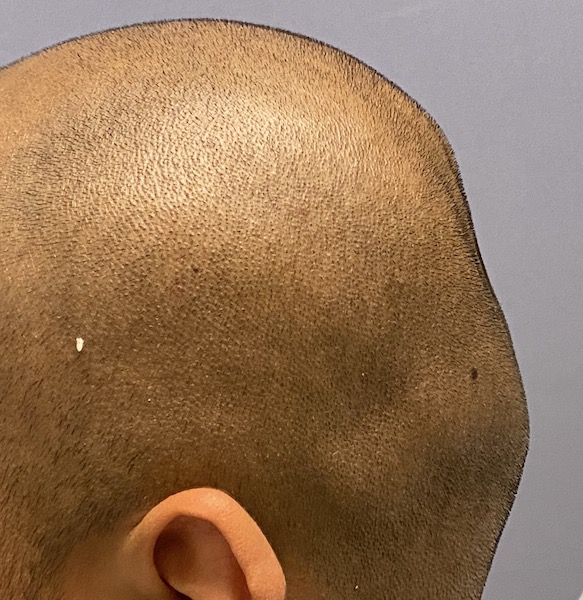
 Case Study: This male had a central occipital flattening which was associated with a slight asymmetry. It also had an irregular contour throughout the back of his head. From the side view it appeared as if a portion of the back of the head was missing.
Case Study: This male had a central occipital flattening which was associated with a slight asymmetry. It also had an irregular contour throughout the back of his head. From the side view it appeared as if a portion of the back of the head was missing.
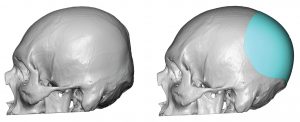 Using a 3D CT scan of his skull a custom implant was designed to increase the direct horizontal projection of the back of his head. To adequately create a smooth contour the footprint of the implant extended past the posterior temporal lines on the sides and up to the crown area on top. With a maximum projection of 13mms a total of 130cc implant volume was obtained. This volume assures that the scalp stretch obtained from a subperiosteal release would allow the implant to fit.
Using a 3D CT scan of his skull a custom implant was designed to increase the direct horizontal projection of the back of his head. To adequately create a smooth contour the footprint of the implant extended past the posterior temporal lines on the sides and up to the crown area on top. With a maximum projection of 13mms a total of 130cc implant volume was obtained. This volume assures that the scalp stretch obtained from a subperiosteal release would allow the implant to fit.
 Under general anesthesia and through an 8cm horizontal long incision placed at the nuchal ridge level, the implant pocket was created with long periosteal releasing instruments. The skull implant was prepared by the placement of 5mm perfusion holes. It was folded, inserted and positioned once inside the pocket based on the known position of the implant to the nuchal ridge per the design.
Under general anesthesia and through an 8cm horizontal long incision placed at the nuchal ridge level, the implant pocket was created with long periosteal releasing instruments. The skull implant was prepared by the placement of 5mm perfusion holes. It was folded, inserted and positioned once inside the pocket based on the known position of the implant to the nuchal ridge per the design.



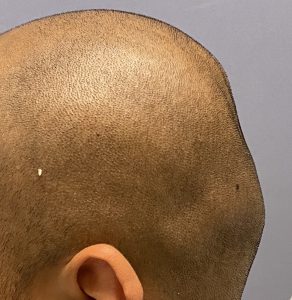
 As would be expected by the design the implant rounded out the back of the head and gave it a much smoother appearance.
As would be expected by the design the implant rounded out the back of the head and gave it a much smoother appearance.
 The most challenging part of placing most custom skull implants is two fold: 1) getting it inserted through a small scar incision, and 2) getting the implant in proper position once inside the pocket and making sure all 360 degree if its edges are fully unfolded. That is challenging because one can only see less than 90 degrees of the implant edges through the small scalp incision. The rest must be done by external feel which is not completely reliable when the scalp tissues are elevated and traumatized.
The most challenging part of placing most custom skull implants is two fold: 1) getting it inserted through a small scar incision, and 2) getting the implant in proper position once inside the pocket and making sure all 360 degree if its edges are fully unfolded. That is challenging because one can only see less than 90 degrees of the implant edges through the small scalp incision. The rest must be done by external feel which is not completely reliable when the scalp tissues are elevated and traumatized.
Case Highlights:
1) Lack of projection of the back of the head can affect it unilaterally (plagiocephaly) or bilaterally. (brachycephaly)
2) In brachycephalic skull deformities it is the occiput that is flat or even indented with surrounding surface irregularities.
3) A custom skull implant provides the most effective treatment of adult brachycephaly whose limits are determined by the stretch of the scalp which is best predicted by preoperative volume of the implant.
Dr. Barry Eppley
Indianapolis, Indiana