


Background: The jaw angle region of the lower jaw has a thick muscular coverage as the insertion of the masseter muscle is along the inferolateral bony border. In a classic example of ‘form follows function’ the shape of the jaw angle bone is a direct reflection of the muscular pull on it. When any type of jaw angle implant is placed for aesthetic augmentation it becomes necessary to perform suberiosteal elevation and lift off most of the lower end of the muscle mass from the bone. In this key technical maneuver of the procedure the muscle elevation must be done around the lower edge of the bone keeping the muscle sling intact.
While the pterygomasseteric muscle relationship of the jaw angle is often described and perceived as a ‘sling’ it actually is not. The muscle fibers of the masseter muscle do not wrap around and intermingle with the muscle fibers of the pterygoid muscle on the other side of the bone. Rather the masseter muscle fibers insert into the periosteum at the inferior border of the bone but do not cross over to the other side. As a result there is only a thin periosteal layer of tissue along its inferior border. This makes release of the inferior border tissues for implant placement a precarious one.

 Should the periosteum along the inferior border become torn during subperiosteal elevation, the most posterior portion of the masseter muscle will retract up over the implant. Postoperatively a contour defect will occur with a thicker muscle layer above a thinner implant region at a 45 degree angle. While this causes no functional jaw movement issues, it is an aesthetic contour distraction that is maximally seen when chewing or clenching one’s teeth.
Should the periosteum along the inferior border become torn during subperiosteal elevation, the most posterior portion of the masseter muscle will retract up over the implant. Postoperatively a contour defect will occur with a thicker muscle layer above a thinner implant region at a 45 degree angle. While this causes no functional jaw movement issues, it is an aesthetic contour distraction that is maximally seen when chewing or clenching one’s teeth.
 Masseteric muscle dehiscence can have variable presentations from mild to severe and its existence is also influenced by whether the implant has a vertical lengthening effect. The anatomically ideal treatment is to reposition the muscle back over the implant…which has variable effectiveness. At the least it requires a neck incision and resultant neck scar.
Masseteric muscle dehiscence can have variable presentations from mild to severe and its existence is also influenced by whether the implant has a vertical lengthening effect. The anatomically ideal treatment is to reposition the muscle back over the implant…which has variable effectiveness. At the least it requires a neck incision and resultant neck scar.
An alternative approach is to leave the muscle where it is and build out the soft tissues over the exposed portion of the implant. This can be done by a variety of techniques from injectable fillers, fat injections to the placement of various types of soft tissue implants.
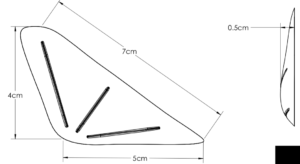
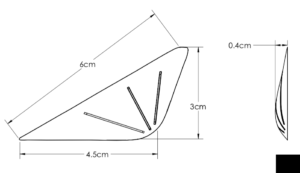 Case Study: This male has a prior history of having a custom jawline implant placed by another surgeon. He developed postoperative masseter muscle dehiscence on both sides, the right being greater than the left. A contouring option was chosen for its correction using ultra soft solid silicone implants whose designs were based on facial measurements of the contour defects.The larger right soft tissue jaw angle implant had a volume of 3.7ccs while the left one was 1.7ccs.
Case Study: This male has a prior history of having a custom jawline implant placed by another surgeon. He developed postoperative masseter muscle dehiscence on both sides, the right being greater than the left. A contouring option was chosen for its correction using ultra soft solid silicone implants whose designs were based on facial measurements of the contour defects.The larger right soft tissue jaw angle implant had a volume of 3.7ccs while the left one was 1.7ccs.



 Under IV sedation anesthesia (he also underwent cheek defatting procedures) and through a small 1 cm skin incision placed directly at the back of the jaw angle, subcutaneous tissue pockets were made and the implants inserted. They were secured with sutures directly to the soft tissue over the very back end of the deeper implant. The skin was closed with small dissolvable sutures and taped.
Under IV sedation anesthesia (he also underwent cheek defatting procedures) and through a small 1 cm skin incision placed directly at the back of the jaw angle, subcutaneous tissue pockets were made and the implants inserted. They were secured with sutures directly to the soft tissue over the very back end of the deeper implant. The skin was closed with small dissolvable sutures and taped.
Soft tissue augmentation using injectable fillers or fat for masseteric muscle dehiscence is either temporary or unpredictable in volume retention. Like on bone an implant in soft tissue offers assured volume/contour retention. But the implant must be very soft for both feel and insertion purposes and must have fine edges to avoid visible edging when healed. Ultrasoft solid silicone fulfills these criteria bit has to be custom made based on measurements of the contour defect.
Case Highlights:
1) The masseter muscle attaches to the bottom of the bony jaw angle region which requires elevation for implant placement.
2) Masseter muscle dehiscence occurs when the insertion of the muscle retracts in varying amounts up over the implant creating a jaw angle contour deformity
3) An ultrasoft solid silicone implant can be designed and placed into the jaw angle soft tissue defect in masseter muscle dehiscence for contour restoration.
Dr. Barry Eppley
Indianapolis, Indiana