

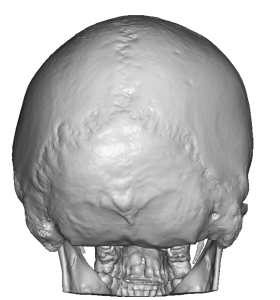
Background: Plagiocephaly is the most recognized and frequently occurring aesthetic skull deformity. While it affects the head overall it greatest aberration in skull shape is posteriorly. Flatness of the back of the head is the sine qua non of plagiocephaly for most patients which is where it is usually seen most significantly.Often called occipital flattening anatomically it is flattening of the triad bony areas of the occipital, parietal and posterior temporal areas. While it is a unilateral deformity and can affect either sides of the back of the head, it is seen far more frequently on the right side in my experience.
The most effective treatment for adult plagiocephaly is onlay augmentation. Bony manipulation via osteotomies is not an option in an adult and only used in infants due their thinner bone and considerable unrealized growth potential. Bone cements are today a poor onlay augmentation option compared to custom skull implant which offer the greater amount of asymmetry correction, an assured predetermined shape and a small scalp incision compared to its size to place it.
In skull augmentations in general aesthetic improvements are always sought of which the most significant one is the scalp incision itself. The goal is always to make the smallest scalp incision that is possible compared to the size of the implant. One technique is a split implant design. This reduces the greatest width of the implant in half which permits a smaller scalp incision to be used. Blindly re-assembling the implant inside the pocket is a challenge but the way the implant is split in the design can help in that regard. Split implant designs can be used in plagiocephaly corrections like any other aesthetic skull augmentation.
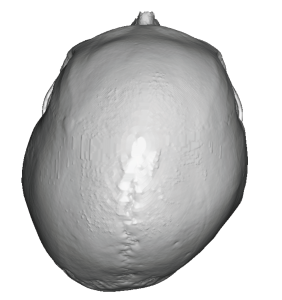
 Case Study: This young male had long been bothered by the right flat side off his head despite having a full head of hair. He self-diagnosed as plagiocephaly and his 3D CT scan confirmed his presence as well as it severity. His right plagiocephaly was significant enough that there was a contralateral left protrusion. But we agreed that trying to burr that side down was not worth the scalp incision needed to do it.
Case Study: This young male had long been bothered by the right flat side off his head despite having a full head of hair. He self-diagnosed as plagiocephaly and his 3D CT scan confirmed his presence as well as it severity. His right plagiocephaly was significant enough that there was a contralateral left protrusion. But we agreed that trying to burr that side down was not worth the scalp incision needed to do it.
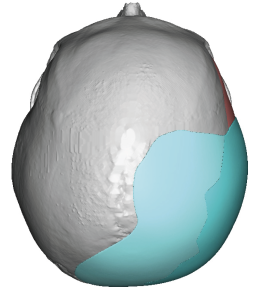
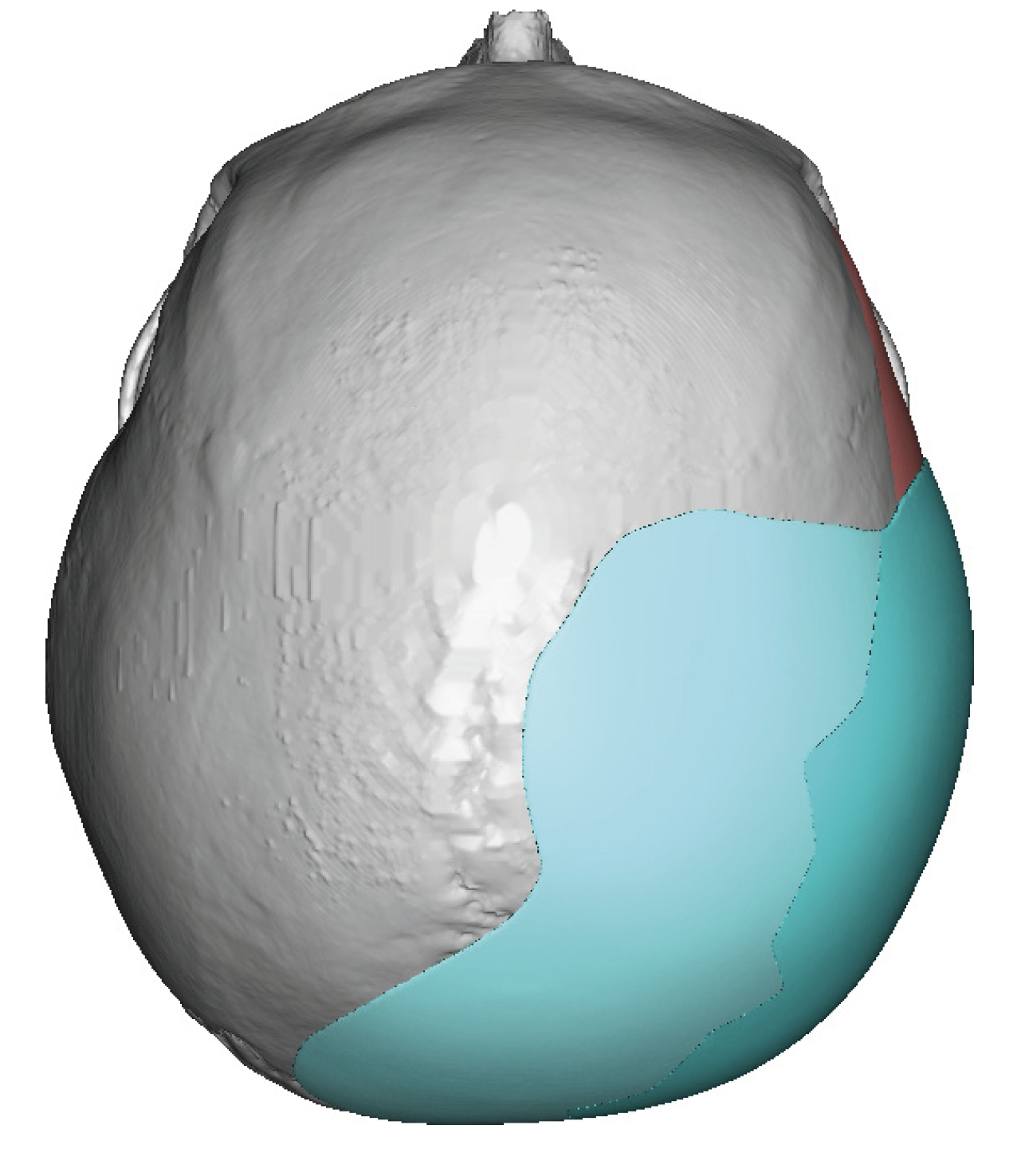
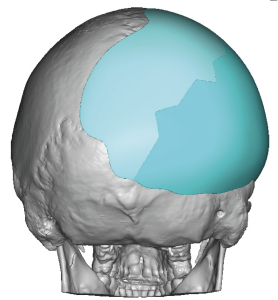 Using his 3D CT scan a skull implant was designed to build out the flatter right side. This required 15mms maximum projection to correct the asymmetry but not be as quite as wide as the left side since it is pushed out a bit.
Using his 3D CT scan a skull implant was designed to build out the flatter right side. This required 15mms maximum projection to correct the asymmetry but not be as quite as wide as the left side since it is pushed out a bit.
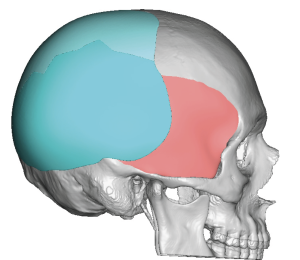 One of the key elements of the implant design is how far it must wrap around the flattened right side well onto the posterior temporal region. (where it sits on top of the deep temporal fascia and not the bone)
One of the key elements of the implant design is how far it must wrap around the flattened right side well onto the posterior temporal region. (where it sits on top of the deep temporal fascia and not the bone)

 Under general anesthesia and in the prone position the position of the implant on the patient’s head could be seen. A small zigzag scalp incision was made which looked remarkably small given the size of the implant.
Under general anesthesia and in the prone position the position of the implant on the patient’s head could be seen. A small zigzag scalp incision was made which looked remarkably small given the size of the implant.

 The skull implant was inserted by first placing the left side half followed by the right side. The two pieces essentially snapped together once inside in which the two halves were secured by sutures and then microscrews at the incision site.
The skull implant was inserted by first placing the left side half followed by the right side. The two pieces essentially snapped together once inside in which the two halves were secured by sutures and then microscrews at the incision site.
 The scalp incision was then closed over a drain.
The scalp incision was then closed over a drain.
Key Points:
1) Plagiocephaly is most associated with flattening of one side of the back of the head usually seen more on the right than the left.
2) Hair can camouflage plagiocephaly to a large degree but that doesn’t eliminate the patient’s insecurity about their head shape.
3) A two-piece custom skull implant can provide good symmetry improvement in the asymmetric back of the head with the smallest scalp incision possible.
Dr. Barry Eppley
World-Renowned Plastic Surgeon