

Background: Aesthetic manipulation of the chin can be done using a variety of implant and bone reshaping techniques. Implants provide various dimensions of augmentation. Bone reshaping is more versatile being capable of both horizontal and vertical increases as well as horizontal, vertical and width reductions. In some patients implants and bone reshaping techniques may be combined to achieve the desired aesthetic result.
With the different chin reshaping methods comes the need for surgical access which can be done either from an intraoral or an external submental skin approach. These incisional approaches come with their own advantages and disadvantages and not all chin reshaping methods can be done through either approach. A sliding geniplasty, for example, can only be done through an intraoral incision. Implants, however, can be done through either incisional technique. One could argue that the submental skin approach is the best implant method as it allows access for any size implant placement and a lower risk of infection.
Some patients who have more than one chin surgery may end up employing a variety of different reshaping methods and incisions.
Case Study: This female had a prior history of an initial sliding genioplasty which she felt was too vertical long and horizontally forward. She also did not like the prejowl indentations which were the result of the advancement of the back end of the osteotomy lines.
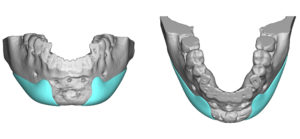
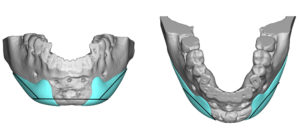
 She subsequently underwent a subtotal sliding genioplasty reversal to bring the chin up and back but not back to its original precut position. In addition custom lateral wing/prejowl implants were made to fill in the bony defects on the side of the chin and create increased width that she preferred.
She subsequently underwent a subtotal sliding genioplasty reversal to bring the chin up and back but not back to its original precut position. In addition custom lateral wing/prejowl implants were made to fill in the bony defects on the side of the chin and create increased width that she preferred.
 Months later, while she liked the improvement, she decided that her chin needed to be still vertically shorter. Rather than take down the sliding genioplasty again, a submental approach was taken to do the vertical reduction. In doing this would also require that the lateral prejowl implants be removed, reduced and replaced.
Months later, while she liked the improvement, she decided that her chin needed to be still vertically shorter. Rather than take down the sliding genioplasty again, a submental approach was taken to do the vertical reduction. In doing this would also require that the lateral prejowl implants be removed, reduced and replaced.

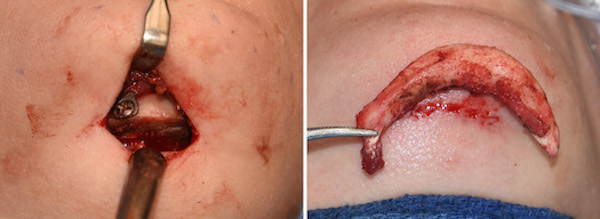
 Through a small submental incision, the custom implants were removed and a horizontal osteotomy was done right at the inferior location of the fixation plate and screws. (5mm vertical chin reduction) The implants were modified/reduced with a scalpel and replaced. A geniohyoid muscle resuspension was then done to the bone.
Through a small submental incision, the custom implants were removed and a horizontal osteotomy was done right at the inferior location of the fixation plate and screws. (5mm vertical chin reduction) The implants were modified/reduced with a scalpel and replaced. A geniohyoid muscle resuspension was then done to the bone.
Being able to do a vertical bony reduction through a submental incision in an aesthetic fashion must apply the concept of the ‘mobile window’. The skin and soft tissues can slide around and move from side to side. This allows a much smaller incision to be used than the length of the osteotomy line would otherwise indicate.
Case Highlights:
1) Vertical chin reduction after a sliding genioplasty and custom lateral prejowl implants is best done through a submental approach.
2) The inferior end of the chin fixation plate is a good marker for maximum bone reduction.
3) Vertical chin reduction by osteotomy can be done through a very small incisions using the skin as a ‘mobile window’.
Dr. Barry Eppley
Indianapolis, Indiana