

Background: The top of the head typically has a smooth convex surface from the front view. While the midline is its highest point it has a gentle slope down to the temporal lines which serve a more acute change onto the side of the head. In the aesthetic peaked head shape the top of the head (sagittal area) appears disproportionately taller than the side areas next to it. (bilateral parasagittal areas) Such a head shape often occurs because the overall head is more narrow and it is the parasagittal areas that are deficient. (the sagittal area is actually of a normal height)
In looking at the peaked head shape how to improve it could be a sagittal height reduction, parasagittal augmentation or a combination of both. This is best determined by doing computer imaging and looking at these three types of head shape changes and letting the patient determine what looks best to them. But when a patient chooses a sagittal ridge reduction the key question is which part of the sagittal ridge needs to be reduced. This is best determined by looking at the head in profile.
The sagittal ridge is the area of the skull that coincides with the original sagittal suture line that runs between the original anterior and posterior fontanelles. It can be divided into an anterior and posterior sagittal ridge which is determined by where the transverse coronal suture line crosses it. The most common sagittal ridge skull deformity is posterior between the crown of the head forward to the coronal suture line. Less commonly is the anterior sagittal ridge that runs from the coronal suture line forward to the upper forehead.

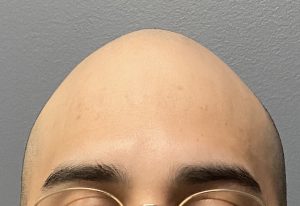
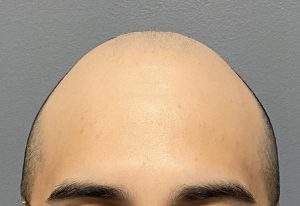
 Case Study: This young male was bothered by a midline prominence on the top of his head that was located on the front half. He had a narrow head shape which magnified the height of the sagittal crest. His 3D skull CT scan showed an anterior ridge from the coronal suture forward. There was no evidence of a sagittal suture line.
Case Study: This young male was bothered by a midline prominence on the top of his head that was located on the front half. He had a narrow head shape which magnified the height of the sagittal crest. His 3D skull CT scan showed an anterior ridge from the coronal suture forward. There was no evidence of a sagittal suture line.
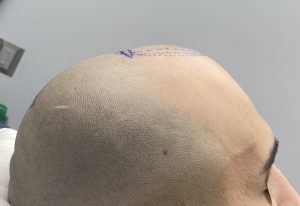
 The anterior sagittal ridge area to be reduced was marked in both length and width with the planned incision at its back end.
The anterior sagittal ridge area to be reduced was marked in both length and width with the planned incision at its back end.

 Under general anesthesia a 3cm horizontal scalp incision was made and the scalp elevated off of the bone over and around the sagittal ridge. This creates a subperiosteal tunnel through which to work. A guarded high speed drill with a long burr is used for the bone reduction.
Under general anesthesia a 3cm horizontal scalp incision was made and the scalp elevated off of the bone over and around the sagittal ridge. This creates a subperiosteal tunnel through which to work. A guarded high speed drill with a long burr is used for the bone reduction.

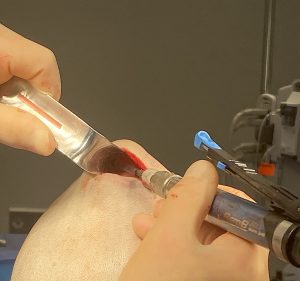 The length of the long burr controls the location of the scalp incision. The incision must be located so that the length of the burr can reach the most anterior point of the sagittal ridge. In this case the incision is located at the coronal suture line at the back end of the ridge as the length of the burr is the same length as that of the bony ridge.
The length of the long burr controls the location of the scalp incision. The incision must be located so that the length of the burr can reach the most anterior point of the sagittal ridge. In this case the incision is located at the coronal suture line at the back end of the ridge as the length of the burr is the same length as that of the bony ridge.
 The ridge is reduced as much as possible, rounding out the sides to prevent creating a flat spot. Closure is done over a drain with a two layer resorbaboe suture closure.
The ridge is reduced as much as possible, rounding out the sides to prevent creating a flat spot. Closure is done over a drain with a two layer resorbaboe suture closure.
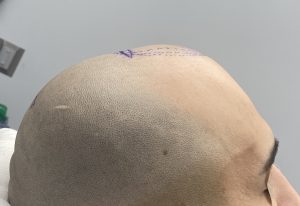
 His immediate intraoperative result showed an adequate reduction of the anterior sagittal ridge. The drain and head dressing are removed the following morning.
His immediate intraoperative result showed an adequate reduction of the anterior sagittal ridge. The drain and head dressing are removed the following morning.

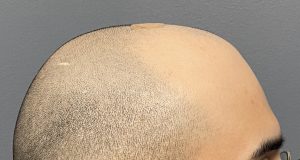 When seen 4 days after surgery prior to returning home he displayed the following result with expected swelling peristence at this early point after surgery.
When seen 4 days after surgery prior to returning home he displayed the following result with expected swelling peristence at this early point after surgery.
Case Highlights:
1) The prominent sagittal ridge can be divided into anterior and posterior ridges separated by the transverse coronal sutures.
2) The location of the incision for sagittal ridge reduction is based on its length vs the length the burr used to reduce it.
3) Visualization through curved retractors and guarded high speed burring are the essential techniques in aesthetic sagittal ridge skull reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon