

Background: One of the most common facial fractures is that of the cheekbone or malar bones. Anatomically this is known as the ZMC or zygomaticomaxillary complex, a name that comes from the four bony legs that support the projection of the cheek bone…the inferior posterior maxillary buttress, the lateral zygomatic arch, the superior lateral orbital rim and the medial infraorbital rim-floor. Blunt trauma causes the prominent cheekbone to fracture along its legs creating a classic depressed cheek fracture pattern.
The ideal time to treat a cheekbone fracture is shortly after it happens and the correct treatment is ORIF (open reduction and internal fixation) to anatomically reposition it. But some of these fractures go untreated either due to not being diagnosed or the patient initially feeling it will not be an aesthetic issue. (swelling initially obscures the depression of the cheekbone) But once the swelling subsides and the overlying soft tissues shrink down around the depressed bone, the flattened cheek becomes apparent.
While treating a depressed cheekbone fracture can be done by breaking the bone again and repositioning it this approach may not be very appealing, particularly if the aesthetic depression is mild. (and there are no other symptoms like infraorbital nerve numbness and/or orbital dystopia) An alternative and often more appealing approach is to leave the cheekbone where it is and camouflage the deformity with an implant overlay.
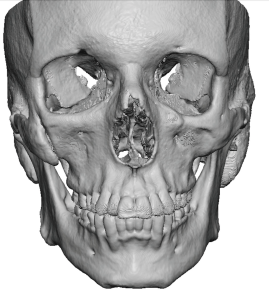
 Case Study: This male had an old left ZMC cheek fracture that was never treated. He disliked the cheek flatness which he periodically treated with injectable fillers. He even tried a right cheekbone reduction to bring the good side in to try and match the depressed side. His 3D CT scan showed a healed but depressed ZMC fracture.
Case Study: This male had an old left ZMC cheek fracture that was never treated. He disliked the cheek flatness which he periodically treated with injectable fillers. He even tried a right cheekbone reduction to bring the good side in to try and match the depressed side. His 3D CT scan showed a healed but depressed ZMC fracture.
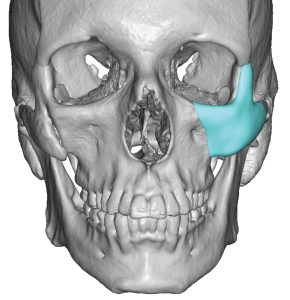
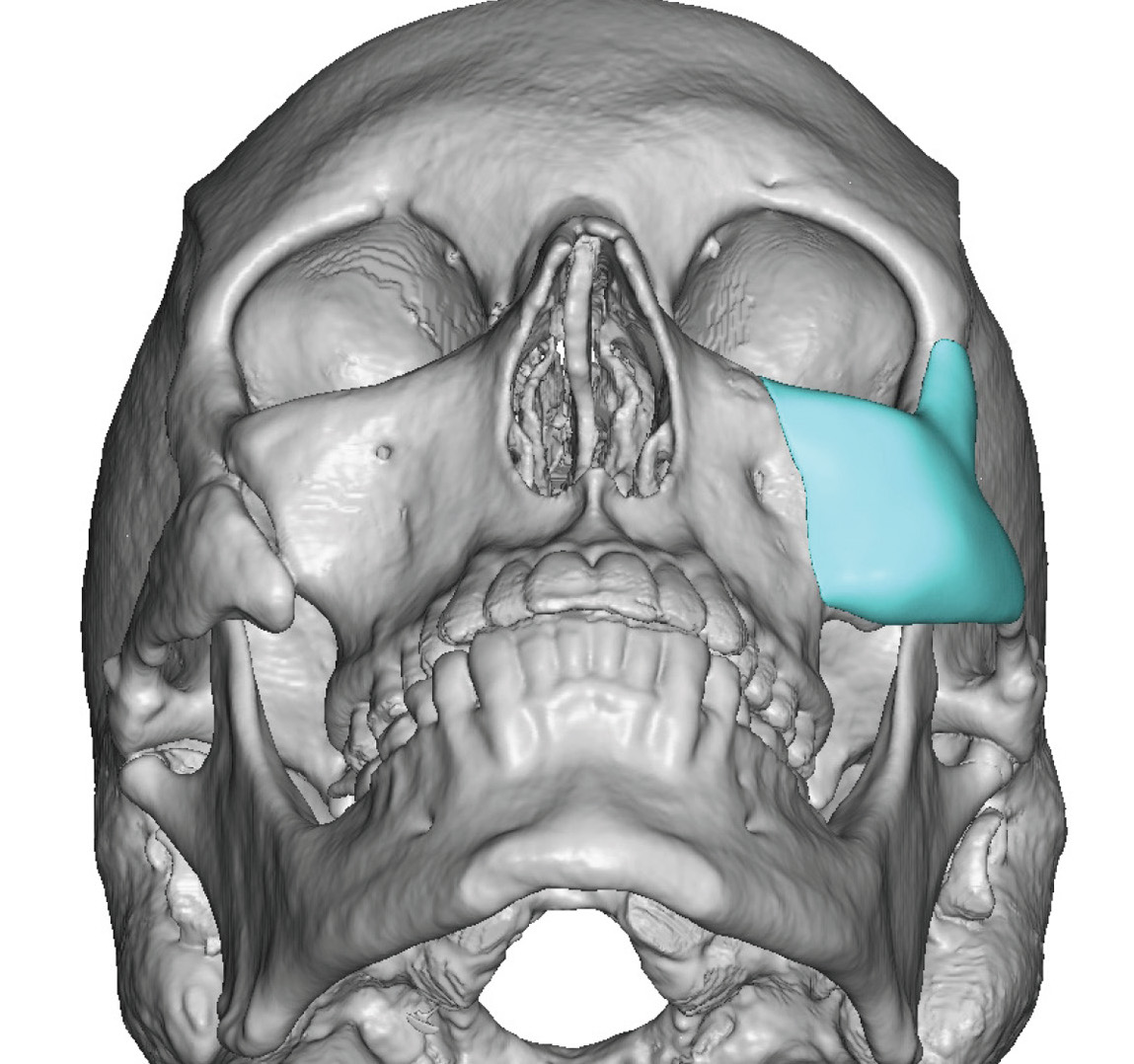
 A custom left cheek implant was designed to match the right cheekbone. It did not extend onto the orbital floor as there was minimal floor lowering.
A custom left cheek implant was designed to match the right cheekbone. It did not extend onto the orbital floor as there was minimal floor lowering.
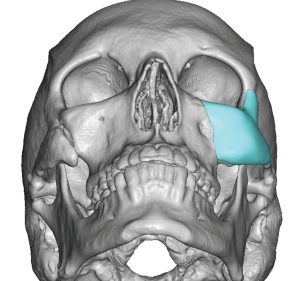
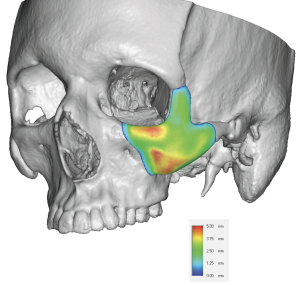 The custom implant had the 3D effect of rotating out the depressed fracture.
The custom implant had the 3D effect of rotating out the depressed fracture.

 Under general anesthesia and through an intraoral approach the scarred soft tissues were widely elevated off the bone. The subperiosteal dissection needed to be carried up to the frontozygomatic suture line superiorly, laterally out onto the mid-zygomatic arch suture and above and medial to the infraorbital nerve.
Under general anesthesia and through an intraoral approach the scarred soft tissues were widely elevated off the bone. The subperiosteal dissection needed to be carried up to the frontozygomatic suture line superiorly, laterally out onto the mid-zygomatic arch suture and above and medial to the infraorbital nerve.
 Once the subperiosteal dissection was adequate so that the implant laid passively on the bone, a single screw fixation was applied into the posterior maxillary buttress.
Once the subperiosteal dissection was adequate so that the implant laid passively on the bone, a single screw fixation was applied into the posterior maxillary buttress.
For a healed cheekbone fracture associated with aesthetic cheek flattening an implant overlay can effectively camouflage the depression. A custom cheek implant approach for the implant design offers the best correction as it matches the shape of the overall depressed bone the best.
Case Highlights:
1) Healed ZMC (zygomaticomaxillary complex) cheekbone fractures can be treated by a custom cheek implant design.
2) A 3D CT scan can clearly show the healed depressed ZMC fracture.
3) Whether the custom cheek implant can be inserted intraorally or through a lower eyelid incision depends on whether there is an orbital floor component.
Dr. Barry Eppley
Indianapolis, Indiana