

Background: Aesthetic augmentation of the orbit is most commonly associated with the standard infraorbital rim or tear trough implant. While effective for the limited problems they are designed to treat, they are unable to affect the vast majority of the orbit rims and other bones attached to it. There is where custom implants and their ability to encompass any aspect the orbital rim and surrounding bones is a game changer for aesthetic periorbital options.
The orbital rim circumferentially surrounds the eye and augmentations of it have been done for selective areas of both the supraorbital rim (brow bones) and the infraorbital rim. But the lateral orbital rim has rarely ever been augmented as the indications for it are not usually recognized. One the primary objectives of orbital rim augmentation is to help the eye that sticks out too far become less prominent. The lateral orbital rim is one of three rim components that can do so.
Since the lateral orbital rim is but very rarely augmented by itself, it is usually done as part of other orbital rim involvement. This could a supralateral orbital rm augmentation if the infraorbital projection is adequate. Or it could be an infralateral orbital rim augmentation if the lateral brow bone has adequate projection. In some cases the ‘three-quarter’ or 270 degree near circumferential augmentation of the orbital rims is to help the appearance of eye pseudoptosis.

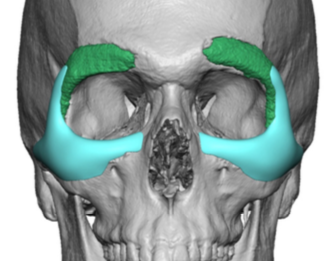
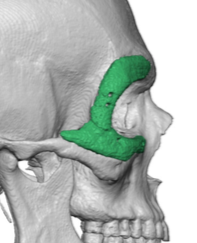 Case Study: This male has a prior history of a custom infraorbital-malar followed by a lateral orbital rim-brow implant for a 270 degree augmentation of his orbits. The objective was to broaden his brow-orbit-cheeks for an overall narrow skull and head shape. Despite these improvements he had finally come to the conclusion that the best and fine improvement would be more lateral orbital rim-malar augmentation.
Case Study: This male has a prior history of a custom infraorbital-malar followed by a lateral orbital rim-brow implant for a 270 degree augmentation of his orbits. The objective was to broaden his brow-orbit-cheeks for an overall narrow skull and head shape. Despite these improvements he had finally come to the conclusion that the best and fine improvement would be more lateral orbital rim-malar augmentation.
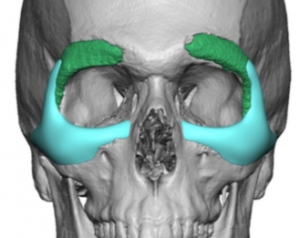
 Using his old 3D CT scan from which his indwelling implants were designed, a replacement custom infraorbital-malar implants was designed with an extended wing along the lateral orbital rim that went up over the existing lateral brow implant.
Using his old 3D CT scan from which his indwelling implants were designed, a replacement custom infraorbital-malar implants was designed with an extended wing along the lateral orbital rim that went up over the existing lateral brow implant.
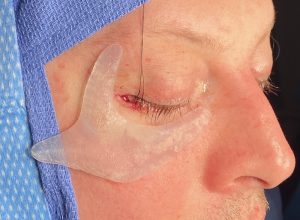
 Under general anesthesia and through his existing well healed and undetectable lower eyelid scars, the old custom infraorbital-malar implants were removed. The comparison of the new implant replacements vs the old implants can be seen when laid side by side.
Under general anesthesia and through his existing well healed and undetectable lower eyelid scars, the old custom infraorbital-malar implants were removed. The comparison of the new implant replacements vs the old implants can be seen when laid side by side.
 To no surprise the size of the new orbital implants with the three long legs made it impossible to place through the size of the lower eyelid incisions.
To no surprise the size of the new orbital implants with the three long legs made it impossible to place through the size of the lower eyelid incisions.

 To place the implants through the lower eyelid incision a vertical geometric split technique was done.
To place the implants through the lower eyelid incision a vertical geometric split technique was done.

 Once inside they were reassembled and a single screw was used for fixation onto the anterior cheekbone. Cheeklifts and lateral canthopexies were done for soft tissue closure.
Once inside they were reassembled and a single screw was used for fixation onto the anterior cheekbone. Cheeklifts and lateral canthopexies were done for soft tissue closure.

 His immediate intraoperative results showed an enhanced fullness to the lateral orbital rim and cheeks but still with a natural appearance.
His immediate intraoperative results showed an enhanced fullness to the lateral orbital rim and cheeks but still with a natural appearance.
Augmenting the orbital rims in a circumferential manner for a precise effect can only be done using a custom implant design. Getting the implants into position is the challenge and various techniques are needed to do so with a limited scarring outcome.
Case Highlights:
1) Widening the narrow facial appearance around the eyes requires augmentation of the outer half of the orbital rims.
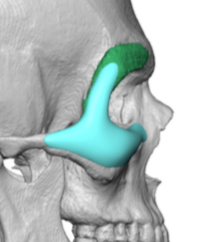
2) The zygomatico-orbital complex is a tripod structure whose inner legs wrap round the infralateral orbital rims while the outer leg heads out onto the zygomatic body and arch.
3) The tripod custom infralateral orbital rim-malar implant can be placed through a lower eyelid incision but may require a geometric split technique to do so.
Dr. Barry Eppley
Indianapolis, Indiana