


Background: Cheek augmentation can be achieved by percutaneous injection techniques or the surgical placement of cheek implants. Of all the facial skeletal areas that can be augmented by injections (synthetic fillers or fat) the cheek area is a particularly effective facial area to do so. This is because the cheeks are softer and not a well defined skeletal area and the more diffuse effects of injection volumes can create a good midfacial enhancement effect. As a result the vast majority of cheek augmentations done today are by injections. Patients usually only graduate to implants when they tire of being injected or desire a unique cheek augmentation effect that injections can not achieve very well.
 The history of cheek implants comes from their uses in females which historically is the most common patient seeking this facial augmentation effect. (Today more men seek cheek augmentation but their aesthetic shape goals are different) It is for this reason that most cheek implant shapes are more oval in form and are designed to be placed partially below the main prominence of the cheek bone. The primary placement error for surgeons is that they think of standard cheek implants as bone implants…which is not accurate. To get the classic more anterior and inferior cheek augmentation effect (the so called apple cheek look) the lower half of the cheek implant must be placed down onto the masseteric fascia. Anatomically this is the same area that is released in a deep plane facelift. By releasing these soft tissue attachments onto the masseteric fascia this could technically be called a deep plane cheek implant.
The history of cheek implants comes from their uses in females which historically is the most common patient seeking this facial augmentation effect. (Today more men seek cheek augmentation but their aesthetic shape goals are different) It is for this reason that most cheek implant shapes are more oval in form and are designed to be placed partially below the main prominence of the cheek bone. The primary placement error for surgeons is that they think of standard cheek implants as bone implants…which is not accurate. To get the classic more anterior and inferior cheek augmentation effect (the so called apple cheek look) the lower half of the cheek implant must be placed down onto the masseteric fascia. Anatomically this is the same area that is released in a deep plane facelift. By releasing these soft tissue attachments onto the masseteric fascia this could technically be called a deep plane cheek implant.
The vexing question in cheek augmentation is always what style and size of cheek implant. This is the one implant procedure where placing various styles of cheek implants on the face helps the patient see the location and the potential effect of the midface augmentation. In women seeking a more profound cheek augmentation the combined malar-submalar shell implant is usually a good selection. More profound or dramatic effects come from the larger sizes of this implant style.
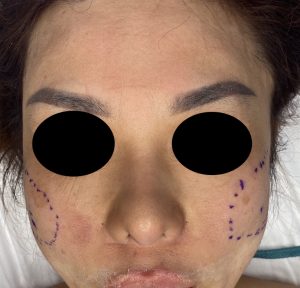
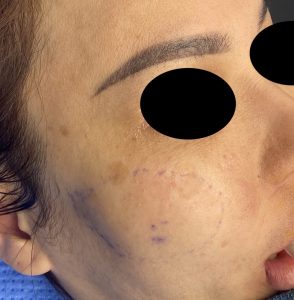
 Case Study: This female had a history of injectable cheek fillers of which some residual filler remained. She wanted an implant approach to lessen the long term costs of cheek augmentation as well as to achieve a more dramatic change that was permanent. While she initially thought that the submalar cheek implant style was what she wanted, between looking at pictures of people who had the cheek look she wanted and placing various styles of cheek implants on her face, the broader coverage malar-submalar shell style was the better choice. The outline of the implants was marked on her face with as much symmetry as possible right before surgery.
Case Study: This female had a history of injectable cheek fillers of which some residual filler remained. She wanted an implant approach to lessen the long term costs of cheek augmentation as well as to achieve a more dramatic change that was permanent. While she initially thought that the submalar cheek implant style was what she wanted, between looking at pictures of people who had the cheek look she wanted and placing various styles of cheek implants on her face, the broader coverage malar-submalar shell style was the better choice. The outline of the implants was marked on her face with as much symmetry as possible right before surgery.


 In surgery through an intraoral approach that involved making the pocket onto the masseteric fascia the cheek implants were placed with single screw fixation to the upper posterior zygomatic buttress. Intraoperatively the immediate cheek augmentation effects can seem ‘extreme’ but it is important to remember how the implant style and size was selected. And as I always ask patients one question about their implant size result before surgery. Short of a perfect result, which side of that result do they prefer…. a bit too small or a bit too big? (In her case she choose a bit too big) This one question will guide whether the intraoperative result seen should be left alone or modified.
In surgery through an intraoral approach that involved making the pocket onto the masseteric fascia the cheek implants were placed with single screw fixation to the upper posterior zygomatic buttress. Intraoperatively the immediate cheek augmentation effects can seem ‘extreme’ but it is important to remember how the implant style and size was selected. And as I always ask patients one question about their implant size result before surgery. Short of a perfect result, which side of that result do they prefer…. a bit too small or a bit too big? (In her case she choose a bit too big) This one question will guide whether the intraoperative result seen should be left alone or modified.
Case Highlights:
1) In using implants for cheek augmentation one must first consider if their desired effect can be done by standard implants or a custom implant approach is needed.
2) The placement of standard cheek implants can be done intraorally with the key maneuver of developing much of the implant pocket onto the masseteric fascia below the cheekbone.
3) For females seeking a dramatic cheek augmentation effect the combined malar-submalar implant style of large sizes can achieve that type of mid facial shape increase.
Dr. Barry Eppley
Indianapolis, Indiana