

Background: Orthognathic surgery has been around for almost 75 years and has evolved in its applications. While one used exclusively when there was an existing malocclusion to realign the dentoaveolar relationships into a more centric bite relationship, its uses has expanded to even when a good occlusal interdigitation exists. (orthodontically created or not) Today bimax double jaw surgery is commonly done for obstructive sleep apnea as well as for aesthetic facial enhancement by bringing the entire lower face forward.
Ideally when a lack of forward growth facial skeletal deficiency exists a bimax procedure should be done initially. Any aesthetic enhancement of the chin, jawline/jaw angles and cheeks can be done secondarily, usually with implants, to build upon the improved skeletal facial foundation. This will also lessen the amount of implant load that is needed to create the final aesthetic facial enhancements. Bimax surgery has a powerful facial effect but is limited to largely a sagittal or 2D change. And it typically can create the need for infraorbital-cheek augmentation as this facial area is left behind above the LeFort I osteotomy line.
But when the need for a Bimax surgery exists but the patient does not want to go through that initial surgery, larger custom facial implants are going to be needed to make up for bone movement that will not be there.
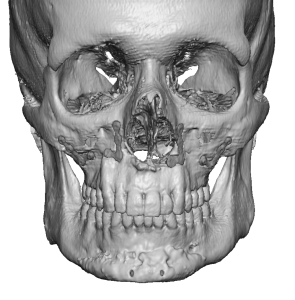
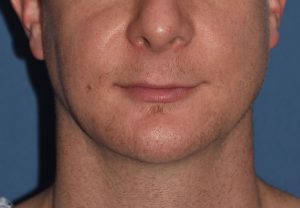
 Case Study: This male presented for a lower jaw augmentation. He had a prior LeFort I osteotomy with a sliding genioplasty. In looking at his face and adjusted orthodontically bite relationship (backward can’t of the upper teeth it was clear that this was not the ideal orthognathic surgical plan. He would have been better served in the long term by a bimax advancement to pull out his facial recession. While he was aware of this facial bone option he did not want to go through a second orthognathic surgical procedure, particularly one of two jaws compared to his first single jaw surgery.
Case Study: This male presented for a lower jaw augmentation. He had a prior LeFort I osteotomy with a sliding genioplasty. In looking at his face and adjusted orthodontically bite relationship (backward can’t of the upper teeth it was clear that this was not the ideal orthognathic surgical plan. He would have been better served in the long term by a bimax advancement to pull out his facial recession. While he was aware of this facial bone option he did not want to go through a second orthognathic surgical procedure, particularly one of two jaws compared to his first single jaw surgery.
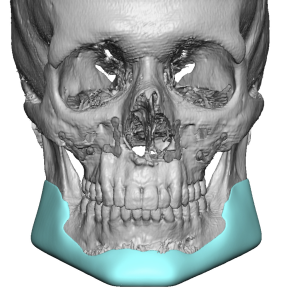
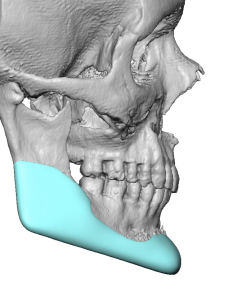
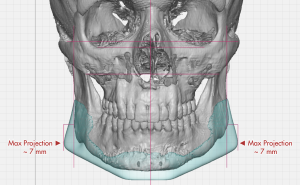
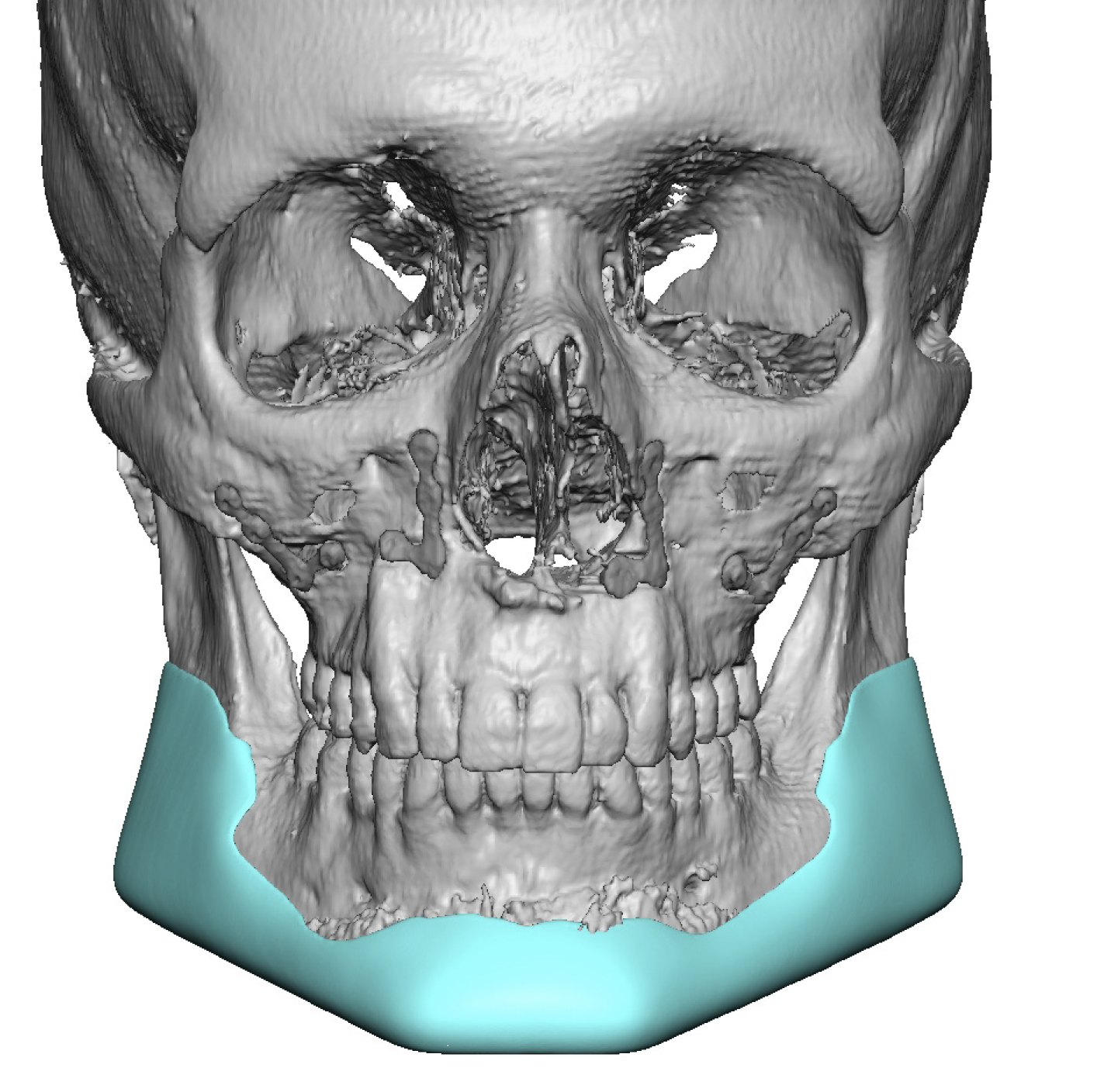
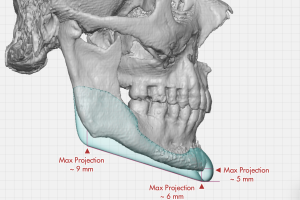 As a result a large custom jawline implant was designed of 24ccs volume. It provided some necessary and significant vertical jawline lengthening along with jawline width and chin projection.
As a result a large custom jawline implant was designed of 24ccs volume. It provided some necessary and significant vertical jawline lengthening along with jawline width and chin projection.
He had the custom jawline implant successfully implanted through the typical three incisional approach. He was doing well and then 6 weeks after surgery developed swelling and some drainage through the submental incision. He was taken back to the OR where the jawline implant was washed out, packed with antibiotic powder and closed. He remains on oral antibiotics for an additional two weeks.
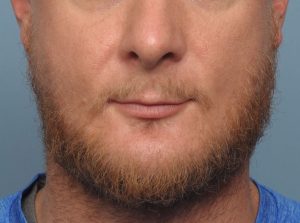



 He was not heard from again for five years when he returned for another unrelated facial procedure. He has remarkably recovered from an infection and remained with his jawline implant in place. It never gave him any problems thereafter the surgical treatment for his infection. His long term result showed the major change to the lower third of his face.
He was not heard from again for five years when he returned for another unrelated facial procedure. He has remarkably recovered from an infection and remained with his jawline implant in place. It never gave him any problems thereafter the surgical treatment for his infection. His long term result showed the major change to the lower third of his face.
Case Highlights:
1) In forward growth facial skeletal deficiencies a bimaxillary advancement is the preferred primary treatment followed by secondary aesthetic implant overlay augmentations if needed.
2) But when the patient is not motivated for that surgery the lower jaw can be augmented by a large custom jawline implant which provides a 3D change.
3) Salvage of an infected jawline implant is rare and this is one of only a handful I have seen that when on to heal uneventful and maintain the implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon