

Background: Cheek augmentation is a common form of aesthetic midface enhancement and uses standard implant styles and sizes to do so. While effective in the properly selected patient, standard cheek implants are inadequate for cheek deficiencies that are more significant in scope, when cheek asymmetry exists or when a specific cheek look is desired. (e.g., high cheekbone look)
Because the eye socket is connected to the cheek bone by both development and anatomic proximity, certain types of cheek deficiencies involve both midface bones. This is most typically seen by the patient as having shallow undereyes or infraorbital hollowing. It is also known as a negative orbital vector. All of which means the anterior position of the bony infraorbital rim and anterior cheek are recessed. With this type of facial skeletal deficiency, the infraornital-malar bony complex needs to be treated for a satisfactory augmentative effect. This can only be done by a custom implant design.
The placement of custom infraorbital-malar implants that have a significant infraorbital component almost always needs to be placed from a lower eyelid approach. It is common to look at the length of these implants vs that of the incision and feel that the implant will not fit through it. But it is really no different than looking at an anatomic chin implant and a small submental skin incision where one can have the same impression. In reality it is not the length of the implant that poses a limitation but its thickness and height that may.
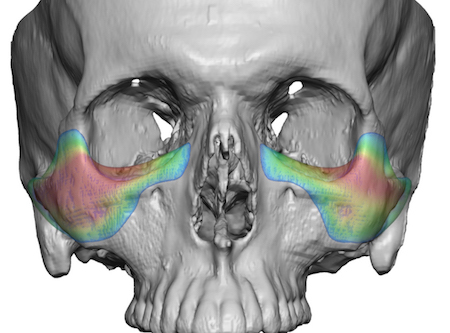
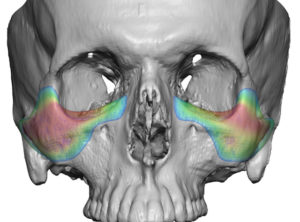
 Case Study: This male had infraorbital hollows and lack of cheek projection with a clinical negative orbital vector. Using his 3D CT scan a custom infraorbital-malar implant design was done that had 5mm of cheek projection, 5mms of vertical infraorbital rim height and 4mms of horizontal infraorbital rim augmentation. There was also a long zygomatic arch component as well as augmentation up along the lateral orbital wall as well.
Case Study: This male had infraorbital hollows and lack of cheek projection with a clinical negative orbital vector. Using his 3D CT scan a custom infraorbital-malar implant design was done that had 5mm of cheek projection, 5mms of vertical infraorbital rim height and 4mms of horizontal infraorbital rim augmentation. There was also a long zygomatic arch component as well as augmentation up along the lateral orbital wall as well.
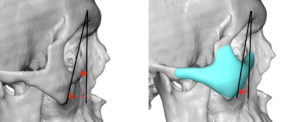 In assessing the implant’s design effectiveness at improving a negative orbital vector, a decrease in the brow-malar profile angle could be seen.
In assessing the implant’s design effectiveness at improving a negative orbital vector, a decrease in the brow-malar profile angle could be seen.


 Under general anesthesia and through lower eyelid incisions, an extended subperiosteal implant pocket was created. But the implant did not fit comfortably through the incision. A geometric split was then made into the implants which enabled them be inserted in two pieces and then reassembled inside and secured with a microscrew one ear side of the split. The incision was then closed after a cheeklift and orbicularis muscle suspension performed.
Under general anesthesia and through lower eyelid incisions, an extended subperiosteal implant pocket was created. But the implant did not fit comfortably through the incision. A geometric split was then made into the implants which enabled them be inserted in two pieces and then reassembled inside and secured with a microscrew one ear side of the split. The incision was then closed after a cheeklift and orbicularis muscle suspension performed.
 Larger custom infraorbital-malar implants can be challenging to place through the limited confines of a lower eyelid incision. But sectioning the implant into two pieces at a location along the infraorbital rim where its reassembly can easily be seen and secured allows even the largest implant to be successfully placed. The reassembly of the implant can be so snugly done that its seam can barely be seen.
Larger custom infraorbital-malar implants can be challenging to place through the limited confines of a lower eyelid incision. But sectioning the implant into two pieces at a location along the infraorbital rim where its reassembly can easily be seen and secured allows even the largest implant to be successfully placed. The reassembly of the implant can be so snugly done that its seam can barely be seen.
Case Highlights:
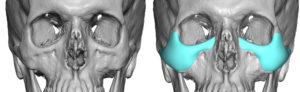
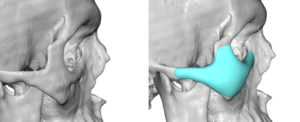
1) Significant infraorbital-malar flattening requires a custom implant design that vertical raises the infraorbital rim as well as augmentation out along the zygomatic arch.
2) Such a large infraorbital-malar implant can the placed through a lower eyelid incision in a geometric split method.
3) Reassmbly of the implant can be done once past the eyelid incision and aligned and secured in place with screws.
Dr. Barry Eppley
Indianapolis, Indiana