

Background: Brow bone reduction surgery today is most commonly associated with transgender facial feminization surgery with the goal being to flatten the brows as much as possible.While not as commonly known brow bone reduction in men has been done for a long time and actually precedes its application in transfemale surgery. What differentiates male vs transgender brow bone reduction are two important issues….aesthetic outcome and incision location options.
Males seek brow bone reduction for abnormally large protrusions or over pneumatized frontal sinus cavities. Their brow bones stick out abnormally with a Neanderthal-type look. Very often the forehead is excessively sloped backward, magnifying the perception of the brow bone protrusion. The goal is to reduce the brow bone prominence to a more normal shape but still have some evidence of a brow bone to maintain a characteristic male facial feature. The brow bone is setback but not to the point where it is completely flat. The outer or tail of the brow is usually left untouched.
Equally important is where to place the incision to access the brow bones in men. While some men have good scalp hair density and a frontal hairline and a superior scalp approach can be used, many men do not. This leaves as the only incision option as a mid-forehead location. While such a location is more known historically in older male browlift surgery it can he equally used in male brow bone reduction…but its length must be limited to well within the interpupillary lines.
Case Study: This male had long been bothered by his prominent brow bones and had many hats to camouflage his forehead appearance. He had lack of any real frontal hairline or top of head hair density. A superior scalp incision was not a good aesthetic option.

 Under general anesthesia a limited mid-forehead incision was marked that corresponded to a wrinkle line…faint as it was. Through this approach the brow bones were completely uncovered by subperiosteal dissection including down onto the frontonasal junction.
Under general anesthesia a limited mid-forehead incision was marked that corresponded to a wrinkle line…faint as it was. Through this approach the brow bones were completely uncovered by subperiosteal dissection including down onto the frontonasal junction.

 The outer table of the frontal sinus (the brow bone mounds between vertical lines drain up through the pupils) was cut and removed using a reciprocating saw and osteotomies. In do doing the brow bone piece fractured and was removed in two pieces. With the bone removed the frontal sinus cavity was fully revealed right down into its entrance into the nose.
The outer table of the frontal sinus (the brow bone mounds between vertical lines drain up through the pupils) was cut and removed using a reciprocating saw and osteotomies. In do doing the brow bone piece fractured and was removed in two pieces. With the bone removed the frontal sinus cavity was fully revealed right down into its entrance into the nose.
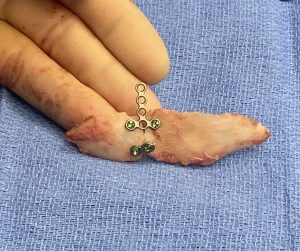 On the back table the removed brow bone was made flatter by burring the inner and outer side and put back together with small 1.5mm plates and 4mm screws.
On the back table the removed brow bone was made flatter by burring the inner and outer side and put back together with small 1.5mm plates and 4mm screws.

 It was put back over the brow bones with some preliminary burring around the edges of the perimeter bone and, once a good position over the sinus was obtained it was secure with single screw fixation to the lower forehead.
It was put back over the brow bones with some preliminary burring around the edges of the perimeter bone and, once a good position over the sinus was obtained it was secure with single screw fixation to the lower forehead.

 The intraoperative changes in brow bone projection were immediately apparent.
The intraoperative changes in brow bone projection were immediately apparent.
Gelfoam collagen sponges were placed around the entire perimeter of the bone flap to cover the small open edges. The incision was then closed with multilayer with resorbable sutures. The incisions was tapped and circumferential head wrap applied. No drain was used as then open underlying frontal sinus provided a source of short term drainage into the nose.

 When seen the next day for head dressing removal, despite the swelling, the brow bone reduction was clearly evident.
When seen the next day for head dressing removal, despite the swelling, the brow bone reduction was clearly evident.
Case Highlights:
1) Male brow bone reduction poses unique incisional challenges because of the frequent lack of a good frontal hairline or top of head hair density.
2) Without a good frontal hairline the only incisional option is a limited mid-forehead wrinkle line location.
3) The male brow bone reduction has a different aesthetic goal than transgender brow bone which is a complete flattening of the brow ridge.
Dr. Barry Eppley
World-Renowned Plastic Surgeon