

Background: The webbed neck is a unique feature of certain genetic disorders. In its fullest expression prominent skin bands exist along the side of the neck with an associated low hairline. A line of hair can be seen to go along the webs at various distances down them. In lesser expressions of neck webbing, usually seen in mosaic patients, more moderate webs exist without hair that runs down along them.
The webbed neck deformity is one of the most challenging of all neck contouring procedures. Unlike almost all other neck contour issues which are anteriorly based below the jawline, the webbed neck occurs on the side of the neck. This location offers no camouflage from either the deformity or any direct type of repair for it.
The webbed neck has been treated by a variety of approaches. The historic technique is a direct one using a line of z-plasties along the webs. While effective this leaves very visible scars on both sides of the neck. More contemporary approaches us a posterior neck technique with variable geometric shapes of excision whose closure pulls the webbing inward decreasing their prominence. This places the scar line in a much more hidden location.
Case Study: This female had very prominent neck webs with a profuse hair density and very low hairline. A line of hair went down along the entire length of the webs. She also had short neck and wide trapezius muscles.

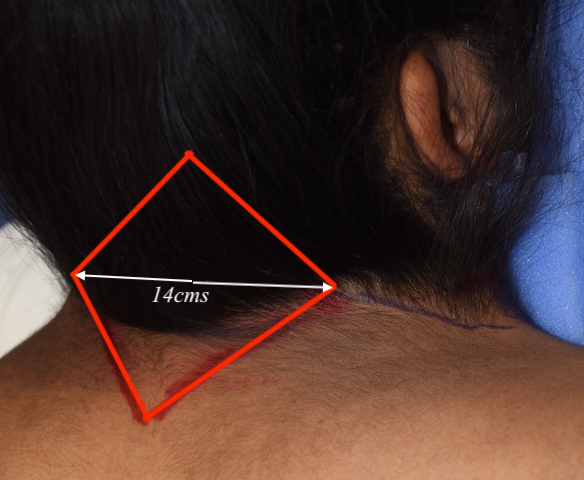
 Under general anesthesia in the prone position, a large diamond-shaped excision was marked with the lateral limbs placed at the horizontal web position where the greatest inward pull could occur. This is determined before surgery with a pinch test on the back of the neck. This horizontal was directly along the bottom of the low hairline. Thus the upper half of the diamond was up into the hairline while the bottom half was on hair-free skin. The diamond excision was carried down through very thick skin and a subcutaneous fat layer down to the muscle fascia.
Under general anesthesia in the prone position, a large diamond-shaped excision was marked with the lateral limbs placed at the horizontal web position where the greatest inward pull could occur. This is determined before surgery with a pinch test on the back of the neck. This horizontal was directly along the bottom of the low hairline. Thus the upper half of the diamond was up into the hairline while the bottom half was on hair-free skin. The diamond excision was carried down through very thick skin and a subcutaneous fat layer down to the muscle fascia.

 A fascial flap was then developed on each side out to within 2 or 3 cms from the muscle border at the web. Midline fascial plication was done to create a deep midline pull on each side of the web.
A fascial flap was then developed on each side out to within 2 or 3 cms from the muscle border at the web. Midline fascial plication was done to create a deep midline pull on each side of the web.
 Large bites of the thick dermis were taken far away from the skin edges to create a second midline closure of pull. The skin was closed without taking any more skin to create a more tension-free closure to minimize the potential for wide scarring. A drain was placed prior to skin closure.
Large bites of the thick dermis were taken far away from the skin edges to create a second midline closure of pull. The skin was closed without taking any more skin to create a more tension-free closure to minimize the potential for wide scarring. A drain was placed prior to skin closure.
The posterior diamond excision to the webbed neck produces maximal inward pull at the most flexible part of the web. It keeps the scar at the most inconspicuous location particularly in longer hairstyles. Such a scar location also provides the opportunity for a secondary procedure if additional web correction is desired.
Case Highlights:
1) Webbed neck deformities are typified by a wide neck due to skin bands that exceed the lateral border of the trapezius muscle.
2) A hidden scar approach to webbed neck improvement employs a posterior neck midline excision with fascial flap plication.
3) Complete webbed neck removal is usually not obtained but substantial improvement in its appearance is.
Dr. Barry Eppley
Indianapolis, Indiana