

Background: Chin implant placement, whether done from a submental or intraoral approach, requires detachment of numerous ligaments from the bone to create the implant pocket. This anatomic necessity has little relevance, and often lack of surgeon awareness, unless the chin implant needs to be removed. The explantation process is far easier than its placement, particularly if it is a silicone implant, and most patients are reassured that the chin will return back to the way it was before surgery.
While the chin snapping back to normal after implant removal seems logical, the soft tissue chin pad is not like a rubber band. This is a failure to understand three basic anatomic sequelae, 1) loss of the chin pad ligamentous attachments, 2) the soft tissue chin pad has been expanded and has limited ability to contract back down, and 3) there is a smooth capsule from the implant both on the bone and on the undersurface of the soft tissue chin pad. Thus once the implant is removed the expanded chin pad falls back with one smooth surface against the other with an inability to stick to the bone.
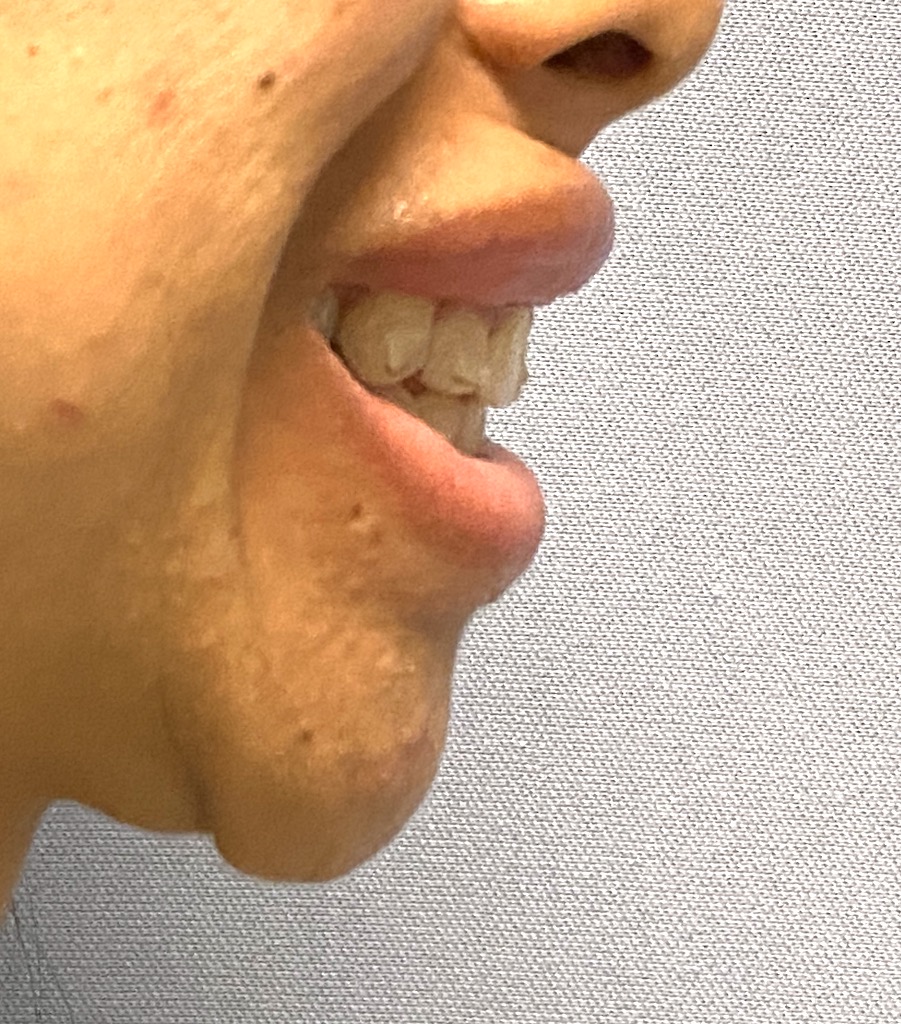
As a result at rest there may be slight evidence of chin pad laxity. But in the patient with right smile pattern (strong lateral pull) the soft tissue chin pad get pulled down creating an large soft tissue overhang. Because it primarily occurs when smiling it is known as dynamic chin ptosis. While it is tempting to try and improve it by resuspension of the chin pad it is important to realize that there is a component of soft tissue excess now.


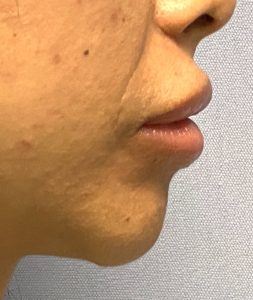
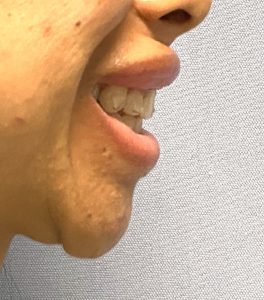 Case Study: This female had a prior history of a silicone chin implant placed through a submental incision. It was subsequently removed as its made her chin too wide. (initial error of using an extended chin implant in a female) Once removed she developed chin pad laxity and a significant dynamic chin ptosis when smiling. Her smile pattern was very strong which made for a large chin pad pulldown.
Case Study: This female had a prior history of a silicone chin implant placed through a submental incision. It was subsequently removed as its made her chin too wide. (initial error of using an extended chin implant in a female) Once removed she developed chin pad laxity and a significant dynamic chin ptosis when smiling. Her smile pattern was very strong which made for a large chin pad pulldown.

 Given her large chin pad overhang a submental approach was taken to treat it. Some of the overhanging chin pad was excised per the markings. This was combined with periosteal suture fixation at three different points of the remaining soft tissue chin pad to the bone.
Given her large chin pad overhang a submental approach was taken to treat it. Some of the overhanging chin pad was excised per the markings. This was combined with periosteal suture fixation at three different points of the remaining soft tissue chin pad to the bone.

 Closure showed a reduced soft tissue chin pad in the static position at the end of surgery. It remains to be seen what its effects will be when smiling.
Closure showed a reduced soft tissue chin pad in the static position at the end of surgery. It remains to be seen what its effects will be when smiling.
The cause of dynamic chin ptosis is the combination of soft tissue excess and loss of ligamentous attachments to hold it up. While intraoral mentalis muscle/chin pad resuspension can be effective for some types of chin ptosis, most cases of dynamic chin ptosis do not do well with it as it can not treat the chin pad excess. The submental technique addresses both of its component causes. The question with the submental approach is not whether it can be effective but to what degree. As the operation is performed under anesthesia (local, sedation or general) the chin pad is not going move/act normally so how much soft tissue pad to remove and how much suture fixation is needed has to be estimated without a precise way to know for sure.
Case Highlights:
1) Dynamic chin ptosis most commonly occurs after chin implant removal due to tissue expansion and detachment of suspensory ligaments.
2) Static chin ptosis frequently occurs as part of dynamic chin ptosis but is usually very subtle.
3) Submental chin pad excision and chin pad fixation is the most effective surgery for dynamic chin pad ptosis.
Dr. Barry Eppley
Indianapolis, Indiana