

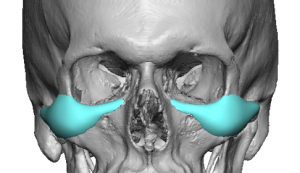
 One of the best custom facial implants, despite being one of the smallest, is the IOM or infraorbital rim implant. It is also one of the most underutilized and unrecognized midface implants. While there are standard cheek as well as tear trough implants for the upper midface, the IOM implant is unique in its aesthetic facial effects. It can provide a complete 3D infraorbital rim augmentation which standard tear trough implants can’t. Its cheek augmentation effects takes it out onto the zygomatic arch which standard cheek implants don’t reach. is also one of the most underutilized and unrecognized midface implants
One of the best custom facial implants, despite being one of the smallest, is the IOM or infraorbital rim implant. It is also one of the most underutilized and unrecognized midface implants. While there are standard cheek as well as tear trough implants for the upper midface, the IOM implant is unique in its aesthetic facial effects. It can provide a complete 3D infraorbital rim augmentation which standard tear trough implants can’t. Its cheek augmentation effects takes it out onto the zygomatic arch which standard cheek implants don’t reach. is also one of the most underutilized and unrecognized midface implants
The two most common uses for IOM implants are in the aesthetic patient who is seeking a high cheekbone look and in the patient with an infraorbital-malar skeletal deficiency best recognized by having a negative orbital vector. Its connected linear shape across the undereye and upper cheek area augments what no bony osteotomy can do. Cheek osteotomies do not change the infraorbital area and LeFort II or III osteotomies do not affect the zygomatic arch cheek areas.
 The surgical placement of IOM implants can be done for two different directions, through an upper eyelid incision or from below through an intraoral approach. As a general rule it is almost always better to do its placement through the lower eyelid particularly if the infraorbital component of the implant saddles the rim and/or there is a significant zygomatic arch extension of it. When these are present the inferior intraoral approach makes it more difficult to get good implant placement as well as the risk of infection and infraorbital nerve numbness is increased.
The surgical placement of IOM implants can be done for two different directions, through an upper eyelid incision or from below through an intraoral approach. As a general rule it is almost always better to do its placement through the lower eyelid particularly if the infraorbital component of the implant saddles the rim and/or there is a significant zygomatic arch extension of it. When these are present the inferior intraoral approach makes it more difficult to get good implant placement as well as the risk of infection and infraorbital nerve numbness is increased.
 The lower eyelid incision needed for IOM pocket dissection and implant placement is a bit different than the traditional eyelid incision used in lower blepharoplasties for aging eyes. It does not need to cross the entire lower eyelid and, more importantly, no tissue is being removed. Thus the orbicularis muscle sling is minimally disrupted which lowers the risk of postoperative lower lid retraction. A lot of dissection can be done through such a small incision using loupes and headlight illumination. Dissection along the infraorbital rim from the lateral orbital rim to the nose is done by direct visualization. Dissection over the cheekbone major is done by direct visualization until the zygomatic arch is reached. Thereafter blind dissection has to be dine using the smart hand technique most commonly used in the placement of cheek implants.
The lower eyelid incision needed for IOM pocket dissection and implant placement is a bit different than the traditional eyelid incision used in lower blepharoplasties for aging eyes. It does not need to cross the entire lower eyelid and, more importantly, no tissue is being removed. Thus the orbicularis muscle sling is minimally disrupted which lowers the risk of postoperative lower lid retraction. A lot of dissection can be done through such a small incision using loupes and headlight illumination. Dissection along the infraorbital rim from the lateral orbital rim to the nose is done by direct visualization. Dissection over the cheekbone major is done by direct visualization until the zygomatic arch is reached. Thereafter blind dissection has to be dine using the smart hand technique most commonly used in the placement of cheek implants.
 IOM implants have a low risk of malposition because 2/3s of the subperiosteal pocket is directly visualized. The working end of the implant, how it sits along or onto the infraorbital rim, is right under the incision where it is well seen. Once in the desired position I always use a single 1.5mm screw for fixation down to the main body of the cheekbone. There really is nowhere for the implant to move or migrate given the size of the pocket to the size of the implant. But the benefit of screw fixation is that it compresses the implant tightly against the bone so the risk of palpable edging is decreased. (which is most relevant along the infraorbital rim part of the implant.
IOM implants have a low risk of malposition because 2/3s of the subperiosteal pocket is directly visualized. The working end of the implant, how it sits along or onto the infraorbital rim, is right under the incision where it is well seen. Once in the desired position I always use a single 1.5mm screw for fixation down to the main body of the cheekbone. There really is nowhere for the implant to move or migrate given the size of the pocket to the size of the implant. But the benefit of screw fixation is that it compresses the implant tightly against the bone so the risk of palpable edging is decreased. (which is most relevant along the infraorbital rim part of the implant.
 Closure of the limited lower eyelid incision requires three layers of resorbable sutures. The two deeper layers (cheek pad resuspension and orbicularis muscle) are done only over the lateral orbital rim area. The skin is closed with meticulously placed 6-0 plain sutures under loupe magnification.
Closure of the limited lower eyelid incision requires three layers of resorbable sutures. The two deeper layers (cheek pad resuspension and orbicularis muscle) are done only over the lateral orbital rim area. The skin is closed with meticulously placed 6-0 plain sutures under loupe magnification.
 Like all facial implants, custom ones notwithstanding, there is the aesthetic need for small incisional access areas. While the size of the IOM implant may seem daunting for the small eyelid incision used to place it, it is really no different than the submental incision for a chin or jawline implant or the retro hairline incision for temporal implants when it comes to the implants vs incision size comparison.
Like all facial implants, custom ones notwithstanding, there is the aesthetic need for small incisional access areas. While the size of the IOM implant may seem daunting for the small eyelid incision used to place it, it is really no different than the submental incision for a chin or jawline implant or the retro hairline incision for temporal implants when it comes to the implants vs incision size comparison.
Dr. Barry Eppley
World-Renowned Plastic Surgeon