

Background: The skull is composed of five surfaces that together make up the total shape of the head. Three of them are pure bony in composition and are sagittal in orientation, the front (forehead), top of the head, and back of the head. The paired sides of the head make up the other two and their underlying bone is covered by the temporal muscles.
Any of these skull surfaces can be aesthetically augmented either individually or over multiple surfaces. Most custom skull implants have a primary surface area of coverage with some extension onto the adjoining skull surfaces to create a natural convex head shape. This is within the implant volume ranges of 150ccs or less. But when significant coverage of one or more of the skull surfaces are needed implant volume appreciably increases which may be beyond the stretch of the scalp to accommodate. This is when a first stage scalp expansion is needed.
Total skull augmentation is when all five surfaces of the skull are augmented to some degree. This may be one single joined implant (placed in pieces but joined together once inside the pocket) or multiple non-joined implants. While five surface skull augmentation may be possible in a patient with no prior implants or a first stage scalp expansion, the implants would have to be fairly thin or low in volume to do so.
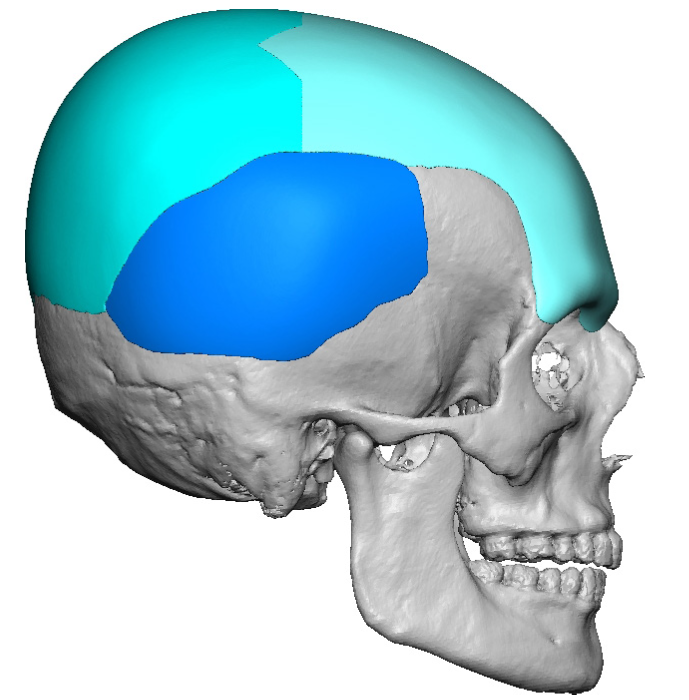
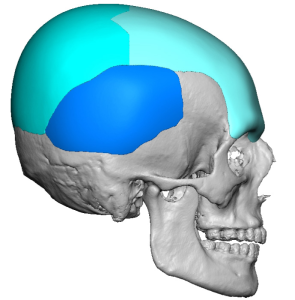
Case Study: This male had a prior custom skull implant across the top and back of his head of 200ccs volume placed years ago. He now desired to add onto it with a forehead-brow implant as well as small temporal implants for a widening effect.
 A custom implant from the brow bones to the back of his head was designed to meet his aesthetic desires of 225ccs. Given its length/size it was known that it could not be placed as a single piece so a split design was made.
A custom implant from the brow bones to the back of his head was designed to meet his aesthetic desires of 225ccs. Given its length/size it was known that it could not be placed as a single piece so a split design was made.
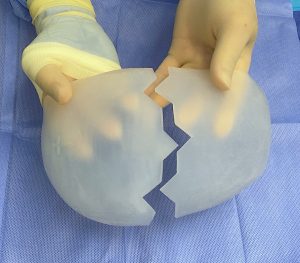
 The key to the split design was that the two pieces are inserted separately and then put together along the split once inside the pocket. This allows the existing scar to stay the same length without extending it.
The key to the split design was that the two pieces are inserted separately and then put together along the split once inside the pocket. This allows the existing scar to stay the same length without extending it.
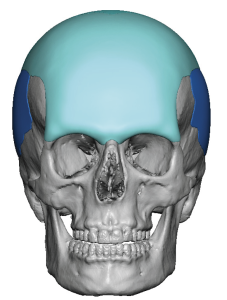
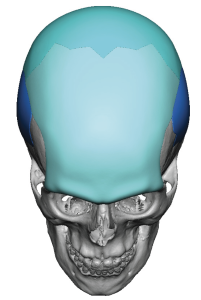
 Small temporal implants (3mm thickness) were also designed to be placed independently of the larger implant.
Small temporal implants (3mm thickness) were also designed to be placed independently of the larger implant.

 Under general anesthesia and through his existing scalp scar the two piece large skull implant was placed. But to get an effective forehead dissection done down to the brow bones a separate small incision was needed just behind the frontal hairline. Through this incision an endoscope was used to see the brow bone releases and protect the supraorbital nerves. Once the front larger implant piece was in good position it was secured with a microcrew through this anterior scalp incision.
Under general anesthesia and through his existing scalp scar the two piece large skull implant was placed. But to get an effective forehead dissection done down to the brow bones a separate small incision was needed just behind the frontal hairline. Through this incision an endoscope was used to see the brow bone releases and protect the supraorbital nerves. Once the front larger implant piece was in good position it was secured with a microcrew through this anterior scalp incision.
 The temporal implants were placed through superior postauricular incisions.
The temporal implants were placed through superior postauricular incisions.
While custom skull implants can be designed to change any or all of the head shape the key considerations in doing so are 1) can the scalp accommodate the implant volume and 2) how to get the implants in place through aesthetically acceptable incisional lengths. This case illustrates how these two key considerations are managed.
Key Points:
1) Custom implant augmentations of the head typically involve one or more skull surface areas unless a first stage scalp expansion is done.
2) Five surface areas augmentations done at the same time are rare and require either scalp expansion or an indwelling skull implant.
3) A front to back skull implant requires a dual incisional approach for placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon