

Background: In the short chin, when significant vertical lengthening is the primary deficiency, the bony genioplasty remains the workhorse for this type of lower facial augmentation. Significant vertical chin lengthening is defined in my experience by greater than 7 mm in most patients. This is based on the restrictions of the overlying soft tissue chin pad when an implant is used to stretch it. Remember that aesthetic augmentation implants created their effect by expansion of the overlying and surrounding soft tissues that cover them.
While an implant can adequately stretch the soft tissue chin pad horizontally out to10 to 12mms hey mms it becomes more challenging to do so when the main effect of the augmentation is vertical. This is because in a horizontal movement the additional soft tissue coverage needed is brought up from the neck. (Tissue recruitment) This is why many horizontal chin augmentations will look a bit vertically longer by this unavoidable becausesoft tissue effect. Conversely when the chin is the lengthened vertically with an implant the soft tissue recruitment must come from the chin pad itself which is far less pliable than that of the submental neck tissues.
When significant vertical chin lengthening is needed in the short lower third of the face the question is always how much lengthening in millimeters is needed. There are a variety preoperative maneuvers to make this determination. One of the most effective ones is the jaw thrust maneuver for the patient to simulate the chin position they want and then measure the distance between the now open incisal edges. When making this measurement it is important to add to it the amount of natural incisal overlap that exist when putting the teeth together. In most patients this is going to be 1 to 2 mm. But in the vertically short chin patient which can be associated with a class II occlusal relationship the overbite may be greater.

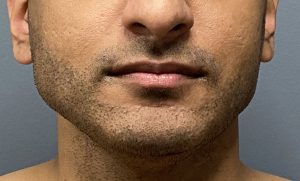
 Case Study: This male had a very short lower third of his face with a near flat mandibular plane angle. Using the jaw thrust maneuver his optimal vertical chin lengthening was more than 10 mm. But because he also needed a few millimeters of increased horizontal projection as well it was elected to keep the vertical lengthening at 10 mm.
Case Study: This male had a very short lower third of his face with a near flat mandibular plane angle. Using the jaw thrust maneuver his optimal vertical chin lengthening was more than 10 mm. But because he also needed a few millimeters of increased horizontal projection as well it was elected to keep the vertical lengthening at 10 mm.
 Under general anesthesia and through and intraoral approach and osteotomy cut was made and the inferior chin segment dropped down. Using a 10 mm plate, which was bent to provide a few millimeters of increased horizontal projection as well as an interpositional tissue bank corticocancellous bone graft the new chin position was secured.
Under general anesthesia and through and intraoral approach and osteotomy cut was made and the inferior chin segment dropped down. Using a 10 mm plate, which was bent to provide a few millimeters of increased horizontal projection as well as an interpositional tissue bank corticocancellous bone graft the new chin position was secured.
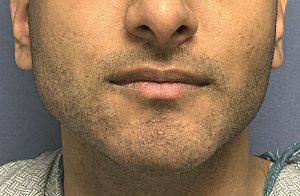 In looking at his one year postoperative result the increased in vertical chin length was evident and the chin shape did not become more narrow. (due to its natural wide shape)
In looking at his one year postoperative result the increased in vertical chin length was evident and the chin shape did not become more narrow. (due to its natural wide shape)

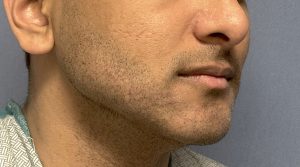 The combined vertical end horizontal dimensional increases could be appreciated in the oblique view.
The combined vertical end horizontal dimensional increases could be appreciated in the oblique view.
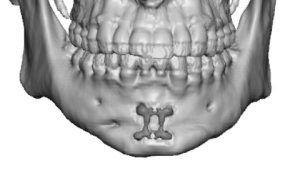
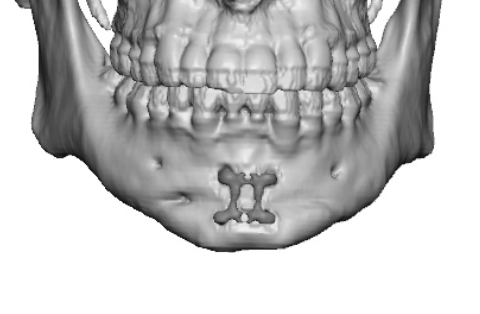
 His postoperative 3-D CT scan shows good bony healing across the open osteotomy gap due to the bone graft that was placed.
His postoperative 3-D CT scan shows good bony healing across the open osteotomy gap due to the bone graft that was placed.
The vertical bony genioplasty remains the primary method of significant elongation of the short lower third of the face. Even if it does not achieve the patience ideal dimensional increases it at least service as the bony foundation if one wants to add an implant later on for a final augmentative and chin reshaping effect.
Key Points:
1) When significant vertical chin lengthening is needed an opening wedge bony genioplasty is the most effective approach.
2) The opening wedge bony genioplasty can also provide some horizontal augmentation as well but will always be less in millimeters than that of the vertical lengthening in the very short chin.
3) A bony genioplasty, particularly when significant movements are done, will not make the chin wider and may make it a bit more narrow in some cases.
4) Having a bony genioplasty does not preclude the potential for secondary additional augmentation with an implant should that be desired.
Dr. Barry Eppley
World-Renowned Plastic Surgeon