

Background
A variety of aesthetic skull deformities exist, some of which are less well known. One such example is the posterior fontanelle skull deformity, located at the site of the original “soft spot” in infancy. This area lies at the intersection of the midline sagittal suture and the paired lambdoid sutures. At birth, it is an open membrane-covered gap between the parietal and occipital bones, but ossification typically occurs within the first three months of life.
In most individuals, bone formation achieves normal thickness. However, in some cases, incomplete ossification leaves a flat spot or indentation, disrupting the normal convex contour of the crown of the skull. For patients who wish to correct this, options include hydroxyapatite cement or a small custom skull implant for minor defects, while larger augmentations require broader reconstruction to enhance overall crown projection.
Considerations in Skull Augmentation
When addressing skull contour irregularities, scalp elasticity is critical. The ability of the scalp to accommodate an implant varies among individuals and is strongly influenced by scalp thickness.
- Thicker scalps (often seen in individuals with darker skin and hair pigmentation) stretch more easily, allowing for larger implants.
- Thinner scalps (such as in light-haired Caucasian females) have limited stretch capacity and are more prone to complications such as hair shock loss, even with moderately sized implants.
For patients with thin, immobile scalps, a tissue expander can be used to gradually stretch the scalp in preparation for implant placement.
Case Study
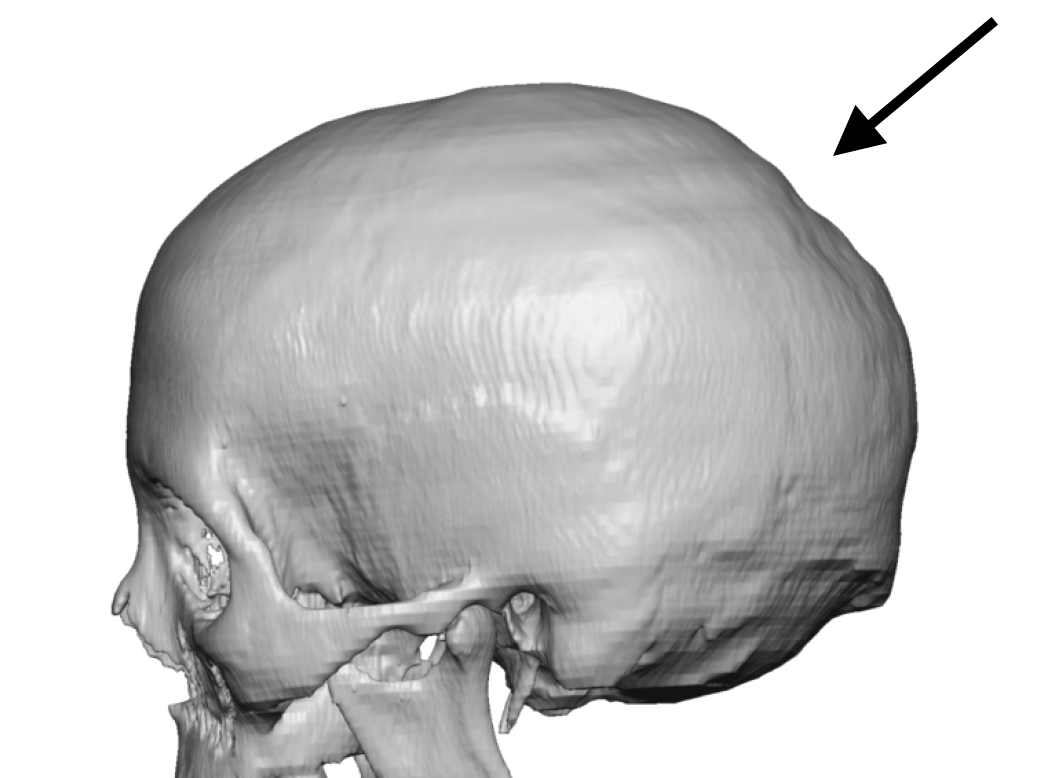
A middle-aged female presented with long-standing concern about a flat area at the crown of her skull over the posterior fontanelle. She had previously styled her hair to camouflage the deficiency but desired a permanent solution.
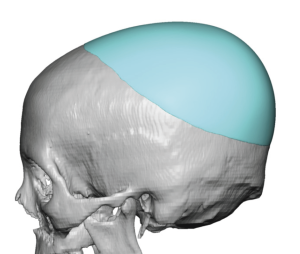 A 3D CT scan confirmed flattening at the crown. A custom skull implant was designed to restore a natural convex contour, adding 19 mm of projection and a total implant volume of 210 ccs.
A 3D CT scan confirmed flattening at the crown. A custom skull implant was designed to restore a natural convex contour, adding 19 mm of projection and a total implant volume of 210 ccs.
Because of her thin, immobile scalp, a first-stage tissue expander was placed and filled to 220 ccs. Unexpectedly, the patient was unable to return for four years for the second stage. Remarkably, the expander remained intact and fully inflated during this time.



 At her return, the expander was removed and replaced with the custom implant through her original incision. Postoperatively, she demonstrated restored crown fullness and elimination of the flat posterior fontanelle defect.
At her return, the expander was removed and replaced with the custom implant through her original incision. Postoperatively, she demonstrated restored crown fullness and elimination of the flat posterior fontanelle defect.
Discussion
Tissue expansion, a technique developed over half a century ago, is highly effective in the scalp because the rigid skull provides a stable platform for expansion. While traditionally used for reconstructive purposes, its application in aesthetic skull augmentation is a logical extension. In this setting, the expander only needs to be filled to the intended implant volume, making it far less noticeable—particularly for women with long hair.
What makes this case unique is the duration of expander placement. While expansion typically lasts 2–3 months, this patient maintained her expander for four years without complications. This durability is consistent with the design of scalp expanders, which share structural similarities with saline breast implants.
Key Points
- A posterior fontanelle skull deformity occurs when the soft spot closes but leaves a flat or indented crown instead of a normal convex shape.
- In thin-scalped Caucasian females, staged scalp expansion is often required before implant placement.
- In this case, a scalp expander remained intact for four years before successful custom implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon