


A sagittal ridge skull reduction refers to contouring down a prominent midline ridge on the top of the skull that follows the sagittal suture. It is usually done for cosmetic reasons when the ridge creates a peaked, narrow, or “keel-shaped” head appearance.
What causes a sagittal ridge?
Common causes include:
- Normal anatomical variation — thickened sagittal suture/ridge without pathology
- Residual sagittal craniosynostosis (treated or untreated)
- Bone overgrowth or asymmetry
Surgical approach
The procedure is usually performed through:

- A very limited coronal scalp incision either at the back end of the sagittal crest or at its midpojnt between the two ends.
Through this small scalp incision:


- Elevates the scalp off the skull creating a ‘tunnel’ for visualization along length of the ridge
- Uses a high-speed burr/drill to reduce the bony ridge, but first a depth cut is made to establish a safe reduction depth
- Smooths and blends adjacent skull contours
- Closes the scalp
Important limitation
The skull can only be reduced to the thickness of the outer cranial bone layer while maintaining safe protection of the brain. So:
- Mild/moderate ridges respond very well
- Severe narrow skull shapes may require broader cranial remodeling rather than simple burring
Recovery
- Outpatient or overnight stay
- Swelling for 1–2 weeks
- Scalp numbness common temporarily
- Return to normal activity in ~2–3 weeks
- Final contour visible after swelling resolves over several months
Risks
- Scalp numbness
- Irregular contour
- Palpable edges
- Bleeding/hematoma
- Infection
- Very rarely dural exposure if aggressive reduction is attempted
Typical candidates
Good candidates usually have:
- Isolated ridge prominence
- Stable skull shape
- Realistic expectations
- Thick enough scalp/hair coverage to conceal incision
How Much Reduction Is Realistically Possible
The realistic amount of sagittal ridge reduction depends almost entirely on the thickness of the outer table of skull bone and the overall head shape.
For isolated sagittal ridges, surgeons can commonly reduce:
- 3–7 mm safely and predictably
- Occasionally up to 8–10 mm in very thick skulls
The limiting factor is that the skull has:
- Outer cortical table
- Diploic space (spongy bone)
- Inner cortical table protecting the brain
Reduction is generally limited to the outer table and part of the diploic layer. You do not want to violate the inner table.
What this means aesthetically
A surprisingly small reduction can make a major visible difference because:
- The ridge catches light/shadow strongly
- The scalp drapes smoother after contouring
- Hair often further softens the contour
So even a 4–5 mm reduction can visually flatten the top of the head substantially.
When simple reduction is enough
Best cases:
- Narrow isolated ridge
- Otherwise normal skull width
- Mild/moderate prominence
These patients often get excellent improvement with burring alone.
When reduction alone is NOT enough
If the head is:
- very narrow,
- boat-shaped/scaphocephalic,
- or globally peaked,
then merely lowering the ridge may not fully change the appearance because the surrounding skull remains constricted.
In those situations, surgeons may discuss:
- parietal augmentation/widening,
- full cranial remodeling,
- or combined reduction + augmentation techniques.
Imaging helps determine limits
A CT scan is the best way to assess:
- bone thickness,
- ridge anatomy,
- and realistic reduction potential.
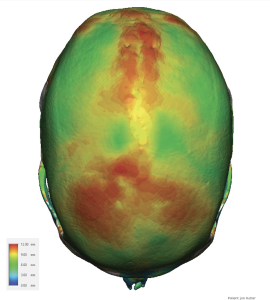
 A 3D CT skull is used preoperatively to measure the bone thickness of the sagittal ridge.
A 3D CT skull is used preoperatively to measure the bone thickness of the sagittal ridge.
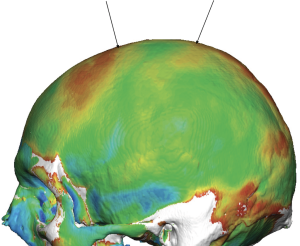
 Cross-sectional analysis can detect any thin spoyts along the desired lone of ridge reduction.
Cross-sectional analysis can detect any thin spoyts along the desired lone of ridge reduction.
Important cosmetic reality
Patients often imagine the ridge can be “completely erased.” In reality:
- The goal is usually softening and blending
- Not creating a perfectly flat skull surface
Trying to over-reduce risks:
- contour irregularities,
- skull thinning,
- or visible depressions.
Dr Barry Eppley
Plastic Surgeon