

Calculating bone thickness in skull reduction (cranial contouring) surgery is a critical step for safety and predictable aesthetic outcomes. Below is a practical, surgeon-focused explanation of how this is done in modern practice.
Primary Assessment Tool: 3D CT Skull Scan
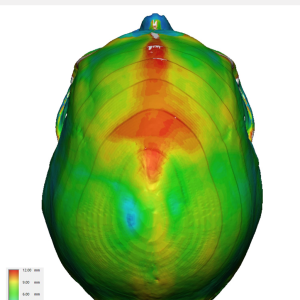
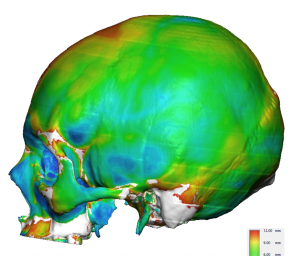
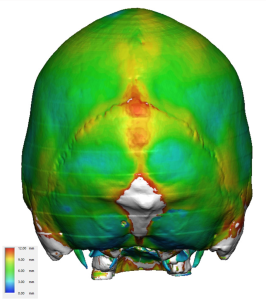
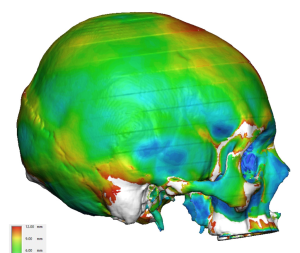 A 3D skull CT scan allows direct measurement of the three layers of the skull, the outer table , diploë, and inner table. While such measurememts could be painstakingly done by serial slicing color mapping provides a more rapid and accurate method for evaluating the bone thicknesses of the entire skull as well as the area to be reduced. It can specifically look for excessively thin areas which may be too thin for safe reduction. It also can show anatomical variations in which an area that may be presumed to be thick actually has thin areas.
A 3D skull CT scan allows direct measurement of the three layers of the skull, the outer table , diploë, and inner table. While such measurememts could be painstakingly done by serial slicing color mapping provides a more rapid and accurate method for evaluating the bone thicknesses of the entire skull as well as the area to be reduced. It can specifically look for excessively thin areas which may be too thin for safe reduction. It also can show anatomical variations in which an area that may be presumed to be thick actually has thin areas.
Measurements are taken perpendicular to the outer cortex at planned reduction sites:
Common Skull Area Typical Bone Thicknesses (Adult)
|
Skull Region |
Average Thickness |
Surgical Notes |
|
Frontal bone (midline) |
6–10 mm |
Diploë often thick |
|
Frontal sinus wall |
2–4 mm |
High-risk zone |
|
Temporal squama |
2–4 mm |
Extremely thin |
|
Parietal bone |
5–8 mm |
Safer for reduction |
|
Occipital bone |
8–14 mm |
Thick but variable |
|
Supraorbital rim |
3–5 mm |
Inner table close |
In skull reduction surgery one can only safely reduce the outer table and part of diploë space. The inner table must remain intact. A safe bone reduction calculation is done by:
- Measure total skull bone thickness (outer ? inner table)
- Subtract minimum inner table safety margin (usually 2 to 3mms)
- Remaining bone = maximum safe reduction
Example:
- Total sagittal crest bone thickness: 9 mm
- Safety margin: 3 mm
- Max reduction: ~6 mm
High and Low-Risk Skull Reduction Zones
 High risk for thinner skull bone thickness areas are:
High risk for thinner skull bone thickness areas are:
- Frontal sinus anterior wall
- Temporal bone
- Pterion
- Supraorbital nerve exit
- Midline upper forehead
 Low risk due to thicker skull bone areas are:
Low risk due to thicker skull bone areas are:
- Occipital bone
- Midline sagittal crest
- Lateral temporal line of frontal bone
Intraoperative Bone ReductionTechnique
 Skull reductions are done by high speed burring (10,000 rpms or less) with a fluted carbide burr. Smoothing is then done by smaller fluted burrs or large skull rasps. While knowledge of the bone thickness of the area to be reduced is essential there are visual cues during surgery to determine the maximum amount of bone that can be safely removed. These include:
Skull reductions are done by high speed burring (10,000 rpms or less) with a fluted carbide burr. Smoothing is then done by smaller fluted burrs or large skull rasps. While knowledge of the bone thickness of the area to be reduced is essential there are visual cues during surgery to determine the maximum amount of bone that can be safely removed. These include:
-
- Change in bone color
- Bleeding diploë
- Sound/feel of burr
- An intraoperative navigation method would be ideal but difficult to apply for bone reductions
Summary
You can safely reduce only what you can measure.
The 3D CT determines the plan; the high speed burr executes it conservatively.
CT imaging determines what is possible.The burr should never discover anatomy you didn’t already measure or know.
Dr. Barry Eppley
World-Renowned Plastic Surgeon