

Pectus excavatum is one of the most recognized of all congenital chest wall deformities. It involves an abnormality of the union and shape of the osteocartilaginous sternum and ribs. It has diverse manifestations that are never the same in any two patients. Due to the emergence of both early and late surgical interventions for its treatment there is also a wide range of presentations of incomplete pectus excavatum corrections as well.
But regardless of its presentation and its history in teens and adults, the end aesthetic goal is the elimination of the sunken chest appearance and improved chest wall symmetry. A variety of treatments have been used for the aesthetic improvement of pectus excavatum from fat grafting, muscle flaps and implants. Of these treatment options implants are the most successful in terms of providing the best chest wall contour augmentation and symmetry improvement.
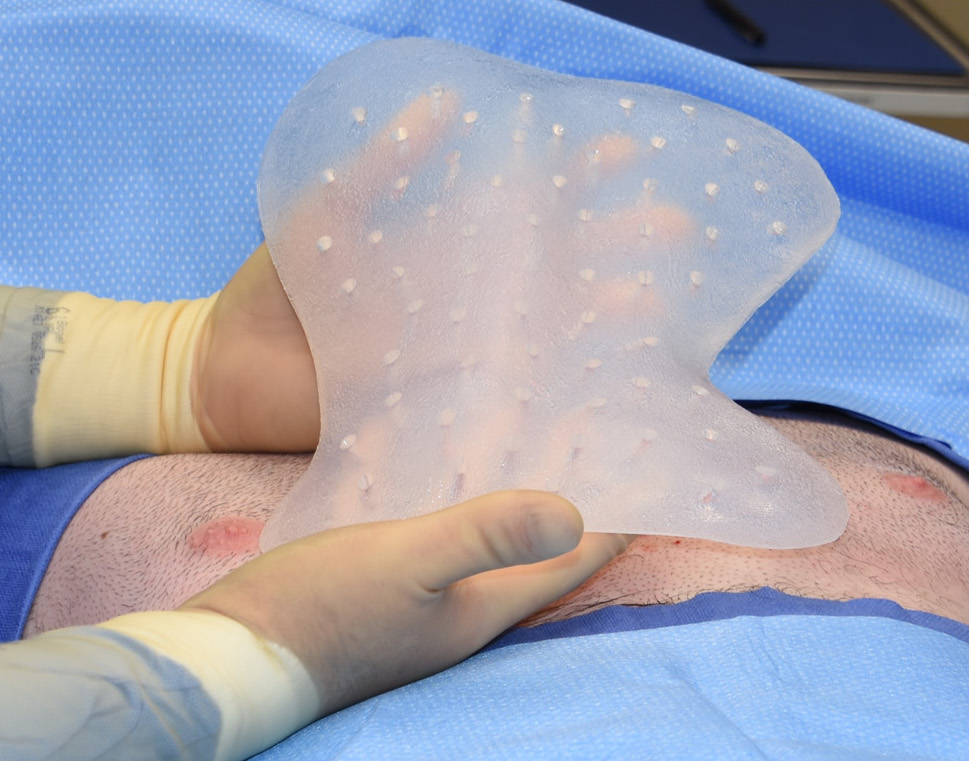 Solid silicone implants are the best material for chest wall augmentation and they are usually placed above the muscle on top of the fascia. Because they are very soft and flexible outside the patient, they can be inserted through relatively small skin incisions to avoid creating an additional aesthetic liability. (big scar).
Solid silicone implants are the best material for chest wall augmentation and they are usually placed above the muscle on top of the fascia. Because they are very soft and flexible outside the patient, they can be inserted through relatively small skin incisions to avoid creating an additional aesthetic liability. (big scar).
 The success of the procedure depends completely on having the proper shape and volume which is going to be different for each patient. The two methods for making custom pectus excavatum chest wall implants is either through the creation of a preoperative moulage or a 3D CT scan. Each methods has their advantages and disadvantages. The moulage method is based on creating a shaped silicone elastomer mold based on the desired external shape which is then translated to a computer design file from which the formal implant is created. This is a more laborious process and requires a surgeon who us facile with the use of these materials.
The success of the procedure depends completely on having the proper shape and volume which is going to be different for each patient. The two methods for making custom pectus excavatum chest wall implants is either through the creation of a preoperative moulage or a 3D CT scan. Each methods has their advantages and disadvantages. The moulage method is based on creating a shaped silicone elastomer mold based on the desired external shape which is then translated to a computer design file from which the formal implant is created. This is a more laborious process and requires a surgeon who us facile with the use of these materials.
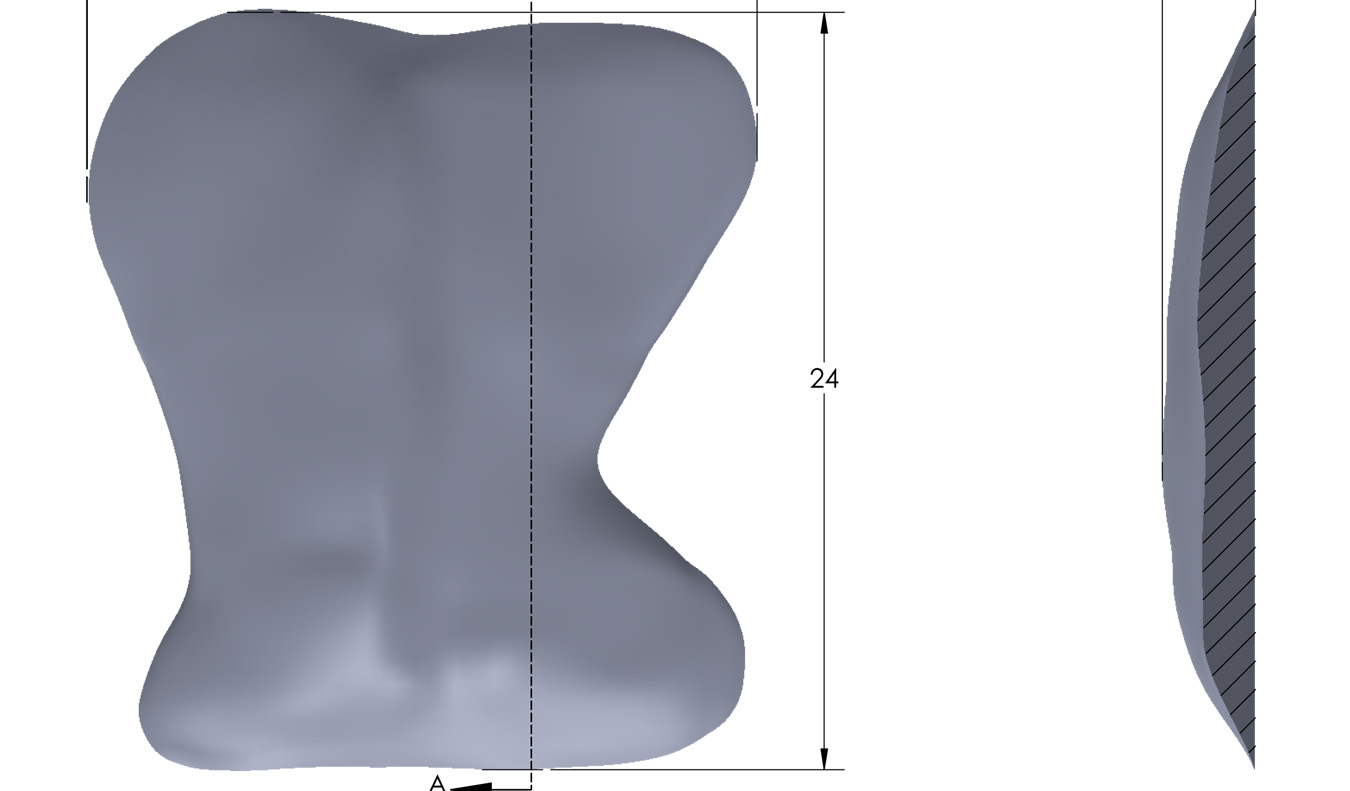
The 3D CT scan method uses a computer designing process based on the patient’s skeletal anatomy and makes an implant based on a corrected skeletal shape. (which may or may not include the pectoral muscles) It is a hand-off method for the surgeon and requires a 3D computer implant designer. Whether the skeletal correction alone provides the best external shape changes presumed but not always assured.
Custom pectus excavatum chest wall implants can be small or remarkably large based on the extent of the deformity and the amount of correction desired. Because the implant sits above the muscle it can cover a large surface area for maximal correction.
Dr. Barry Eppley
Indianapolis, Indiana