

Reconstruction of the skull can be done using a variety of alloplastic materials. Over the years synthetic cranioplasties have evolved from solid metal plates to bone cements to computer-generated implant replacements of lost bone. While some techniques are most historic than others, each still has a role to play in contemporary cranioplasty surgery.
When there js adequate time to have a 3D computer-generated implant reconstruction done, this is almost always the preferred method for large full-thickness skull defects. The strength of the materials (HTR, PEKK, PEEK) and their exacting fit makes them as ideal as possible for a non-autogenous reconstruction.
But when time does not permit the necessary fabrication time for a 3D implant, several alternatives exist. One option is that of bone cement. While there are several different types of bone cements, they will require a backing for their use in large full-thickness skull defects. The hydroxyapatite bone cements, in particular, do not have enough strength when wet to resist displacement and potential fracture. Even with traditional PMMA bone cements, a rigid backing is still structurally beneficial
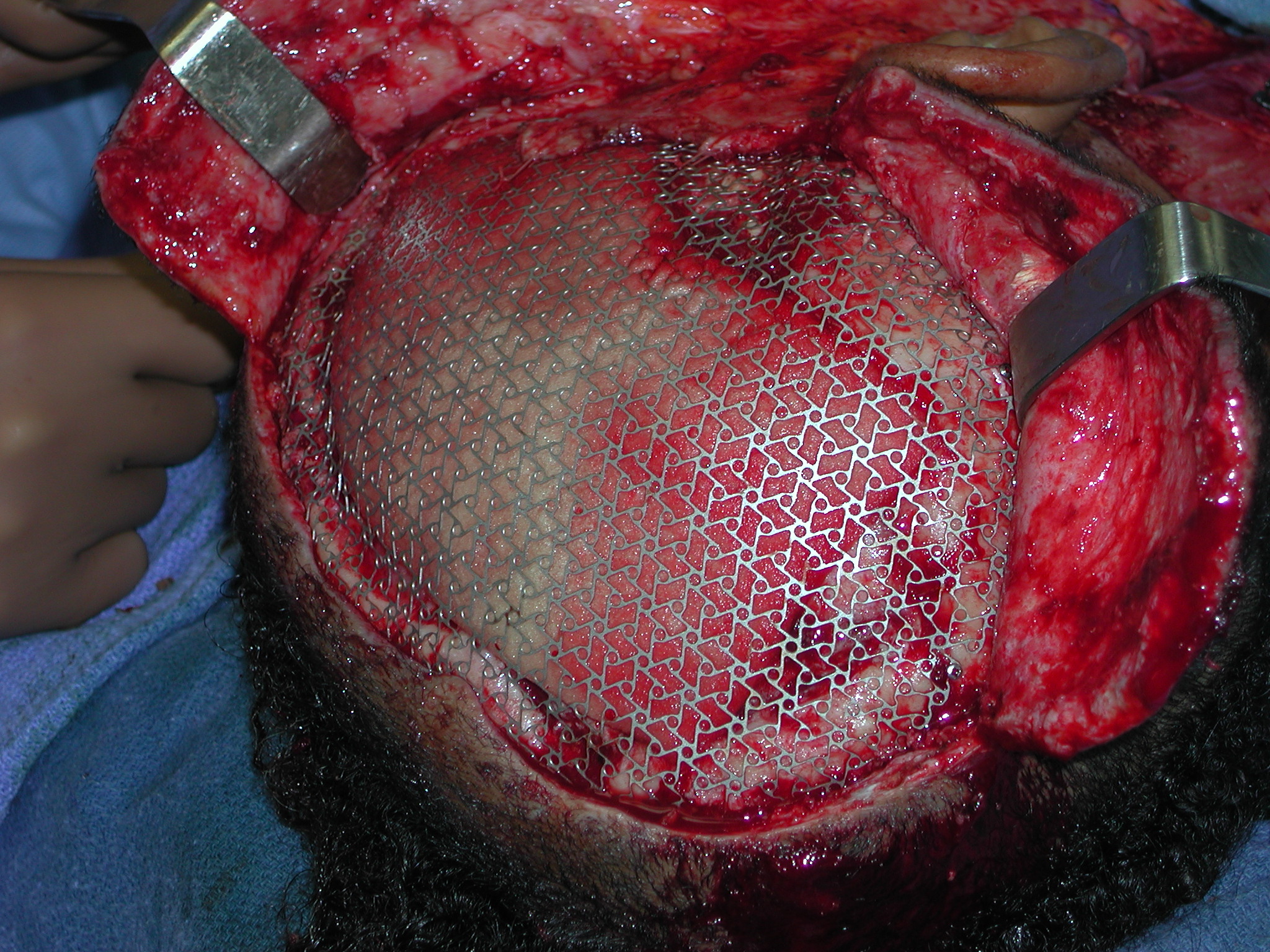 The best intraoperatively fashioned backing for full-thickness skull defects is titanium mesh. It comes in a variety of geometric configurations. But the hexagonal pattern allows for the most malleability of its shape and adaptation to the surrounding bone edges. It also has a lot of metallic edges onto which bone cements can grab onto in the setting and curing process of the material.
The best intraoperatively fashioned backing for full-thickness skull defects is titanium mesh. It comes in a variety of geometric configurations. But the hexagonal pattern allows for the most malleability of its shape and adaptation to the surrounding bone edges. It also has a lot of metallic edges onto which bone cements can grab onto in the setting and curing process of the material.
While traditional metal cranioplasty refers to an outer solid cover over the defect, a mesh metal cranioplasty refers to its use as a backing for bone cement materials. If a mesh material is placed in the outer surface of the bone alone, tissue contraction around its mesh shape will eventually reveal these irregularities particularly in the exposed forehead area.
Dr. Barry Eppley
Indianapolis, Indiana