


Of all aesthetic arm implants that are placed, the most common is that of the biceps muscle. Technically known as the biceps brachii, because of its two muscle heads, it is perceived on the outside as a single muscle…which it ultimately becomes at the mid-upper arm level and as it approaches and attaches into the forearm. The biceps muscle is unique because it crosses two joints, both the shoulder and at the elbow.
![]() In placing biceps implants there are two incisional and pocket locations of which to choose. The most common in my experience is the axillary incisional approach with a subfascial implant location. This approach offers a ‘hidden’ axillary incision, a very direct approach to the subfascial plane with no risk of nerve injury and the ability to place larger implants. The recovery does seem to faster and the aesthetic effect reveals the full volume and shape of the implant.
In placing biceps implants there are two incisional and pocket locations of which to choose. The most common in my experience is the axillary incisional approach with a subfascial implant location. This approach offers a ‘hidden’ axillary incision, a very direct approach to the subfascial plane with no risk of nerve injury and the ability to place larger implants. The recovery does seem to faster and the aesthetic effect reveals the full volume and shape of the implant.
The disadvantages of the subfascial biceps pocket is the risk of implant asymmetry (off the longitudinal axis of the muscle) and disruption of the distal fascia with implant show and potential pain.

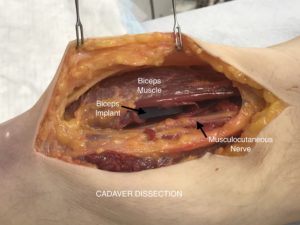 The other biceps implant location is submuscular. This requires a small medial arm incision with a direct dissection down between the muscle and the humerus bone. It provides a smaller pocket than the subfascial location but offers complete muscular coverage and a ow risk of implant displacement. As a result of the incision location it is necessary to pass right over the musculocutaneous nerve in the dissection between the skin and the bone. As a result there is a low risk of nerve injury which would present as numbness or tingling over the side of the forearm. The musculocutaneous nerve is fairly large and is easily seen during the dissection so any injury would be that related to stretch which should recover.
The other biceps implant location is submuscular. This requires a small medial arm incision with a direct dissection down between the muscle and the humerus bone. It provides a smaller pocket than the subfascial location but offers complete muscular coverage and a ow risk of implant displacement. As a result of the incision location it is necessary to pass right over the musculocutaneous nerve in the dissection between the skin and the bone. As a result there is a low risk of nerve injury which would present as numbness or tingling over the side of the forearm. The musculocutaneous nerve is fairly large and is easily seen during the dissection so any injury would be that related to stretch which should recover.
The two options for biceps implant placement have their advantages and disadvantages. Patients will understandably ask which one is better and the answer is…it depends. If I was doing pectoral implants at the same time I would use the same incision to create a subfascial pocket for the implants. If arm implants were done by themselves that would be one reason to consider the medial arm approach.
Dr. Barry Eppley
Indianapolis, Indiana