

The labiomental fold is the natural indentation between the lower lip and the chin. It usually is about 1/3 the distance between the lip and chin, being closer to the lip than that of the chin. It represents the attachments of the mentalis muscle to the underlying bone (its origin) and is also reflective of the resultant depth of the intraoral vestibule between the lower lip and the teeth.
Its depth is dependent on many factors from natural development including the lower lip-tooth relationship and the bony projection of the chin. But it can also be caused to become deeper by aesthetic chin augmentations procedures where the labiomental fold above the chin is ‘left behind’ regardless whether the chin bone is cut and moved or whether an implant is used. It can also get deeper and suffer uncomfortable tightness from intraoral access to the chin, particularly if it has been done multiple times.
Creating a less deep labiomental fold and/or releasing its tightness can be done by a variety of methods. Injectable fillers and fat and various subcutaneous implants have been used, all with varying amounts of success. The most effective method to use, in my experience, for severe and refractory labiomental fold issues is a dermal-fat graft. Placed through the mouth at the subcutaneous level right under the skin, it produces the most profound release of the fold and without interfering with the mentalist or orbiculares muscles.
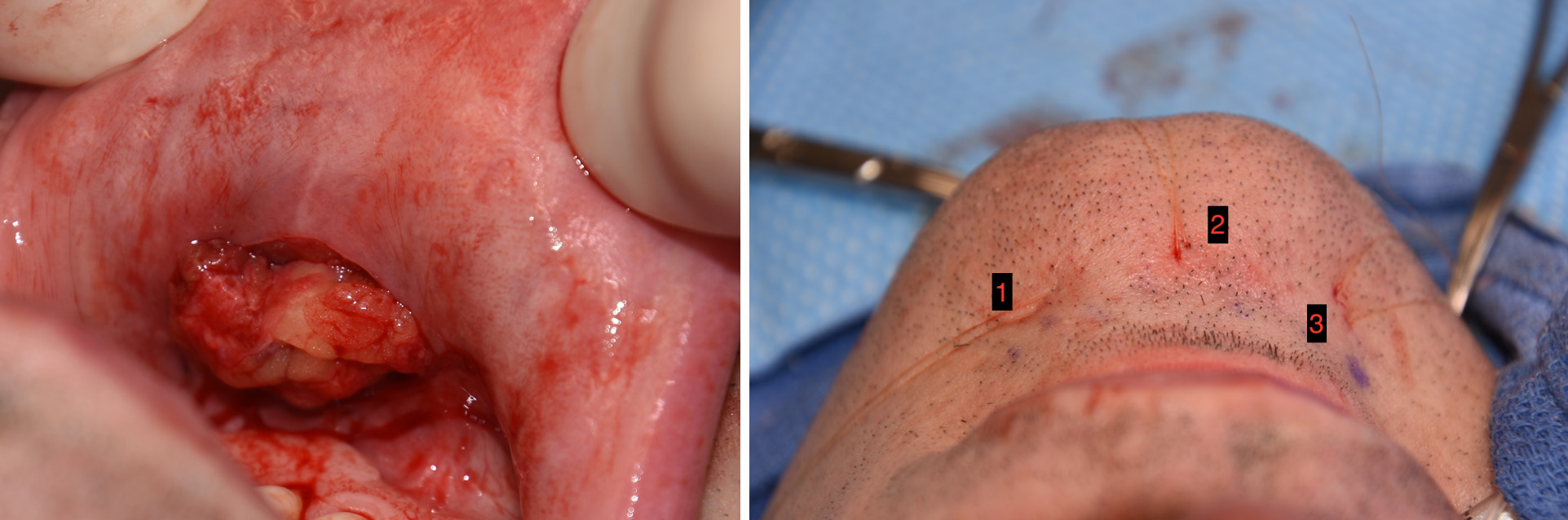 While a dermal-fat graft is a composite graft that is loosely held together by its thin dermal component, getting it into the dissected pocket in the right orientation is not easy. To aid placement the use of three percutaneous bolster sutures is essential. These sutures grab the dermis of the graft at both ends as well as the middle and pulls the graft into the pocket by putting traction on the sutures externally. (passed from the outside in, through the graft’s dermis and then back out to the outside) This also allows the graft to be stretched out over its length with the dermis side up against the underside of the skin along the labiomental fold.
While a dermal-fat graft is a composite graft that is loosely held together by its thin dermal component, getting it into the dissected pocket in the right orientation is not easy. To aid placement the use of three percutaneous bolster sutures is essential. These sutures grab the dermis of the graft at both ends as well as the middle and pulls the graft into the pocket by putting traction on the sutures externally. (passed from the outside in, through the graft’s dermis and then back out to the outside) This also allows the graft to be stretched out over its length with the dermis side up against the underside of the skin along the labiomental fold.
The percutaneous sutures are left in place as the intraoral wound is closed over the fat graft. The sutures can be loosely tied down and removed in a few days or removed cut off at the skin level at end of the procedure.
The most successful dermal-fat grafts to the labiomental fold requires good placement over the length of the fold to ensure an even release.
Dr. Barry Eppley
Indianapolis, Indiana