

Facial lipoatrophy is a well known condition where fat is lost in the face. This occurs at both the subcutaneous level as well as to the deeper buccal fat pad in particular. There are multiple causes and degrees of presentations of it. In its most severe form (often called a level 5 facial lipoatrophy) the face is essentially skeletonized with the skin virtually adhering to the underlying bone. Historically such level 5 facial lipoatrophies were due to drug effects that caused a unique facial fat wasting effect.
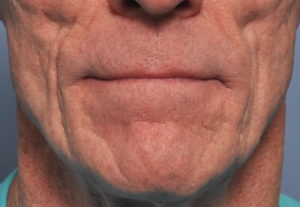 In the treatment or revoluminization of the all forms of facial lipoatrophy, injection treatments are the most commonly used and usually the most effective. From various forms of synthetic fillers to fat, injection placement of volume has a low risk and placement can be very exact. But in the severest forms of facial lipoatrophy the skin is more adhered particularly in the v-shaped nasolabial fold that is usually present. The indention beneath the inferior surface of the cheekbone is where the greatest surface contour depression occurs. This is a good indication for submalar cheek implants to provide a good outward push on the thin contracted overlying tissues.
In the treatment or revoluminization of the all forms of facial lipoatrophy, injection treatments are the most commonly used and usually the most effective. From various forms of synthetic fillers to fat, injection placement of volume has a low risk and placement can be very exact. But in the severest forms of facial lipoatrophy the skin is more adhered particularly in the v-shaped nasolabial fold that is usually present. The indention beneath the inferior surface of the cheekbone is where the greatest surface contour depression occurs. This is a good indication for submalar cheek implants to provide a good outward push on the thin contracted overlying tissues.
 An alternative strategy for these severe cases of facial lipoatrophy is to place an autologous soft tissue graft right beneath the skin in the submalar area using direct incisional access. A dermal-fat graft is an ideal tissue graft as it replaces what has been lost. (fat) The survival rates of dermal-fat grafts in my experience is very high particularly in the face. The deep nasolabial groove is an ideal place for an incision since it is really just like a scar already. The abdomen provides a good location to harvest enough graft for both sides of the face.
An alternative strategy for these severe cases of facial lipoatrophy is to place an autologous soft tissue graft right beneath the skin in the submalar area using direct incisional access. A dermal-fat graft is an ideal tissue graft as it replaces what has been lost. (fat) The survival rates of dermal-fat grafts in my experience is very high particularly in the face. The deep nasolabial groove is an ideal place for an incision since it is really just like a scar already. The abdomen provides a good location to harvest enough graft for both sides of the face.

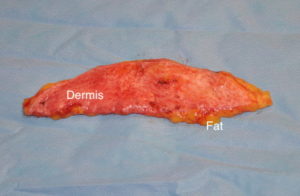
 Using the length of the nasolabial groove for the incision a skin flap which releases the indentation is raised over the desired area of midface augmentation. Raising the skin flap right at the level of the dermis stays safely away from any of the buccal branches of the facial nerve. The dermal-fat graft is placed into the defect with the dermis side up.
Using the length of the nasolabial groove for the incision a skin flap which releases the indentation is raised over the desired area of midface augmentation. Raising the skin flap right at the level of the dermis stays safely away from any of the buccal branches of the facial nerve. The dermal-fat graft is placed into the defect with the dermis side up.
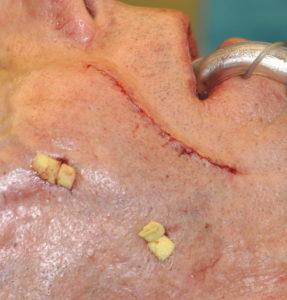 The graft is secured into place by internal sutures where possible and external percutaneous bolster placement at the superior and lateral extent of the graft placement. (where placing internal sutures may risk injuring branches of the buccal facial nerve) The nasolabial fold incision line is closed with subcuticular suturing. The external skin bolsters are removed in 3 to 5 days after surgery.
The graft is secured into place by internal sutures where possible and external percutaneous bolster placement at the superior and lateral extent of the graft placement. (where placing internal sutures may risk injuring branches of the buccal facial nerve) The nasolabial fold incision line is closed with subcuticular suturing. The external skin bolsters are removed in 3 to 5 days after surgery.
The dermal-fat graft provides direct release and volume fill at the deepest part of the facial lipoatrophy. While an invasive surgical procedure its immediate volume fill and high rate of survival makes this a good treatment option for the cheek area of the level 5 facial lipoatrophy patient.
Dr. Barry Eppley
Indianapolis, Indiana