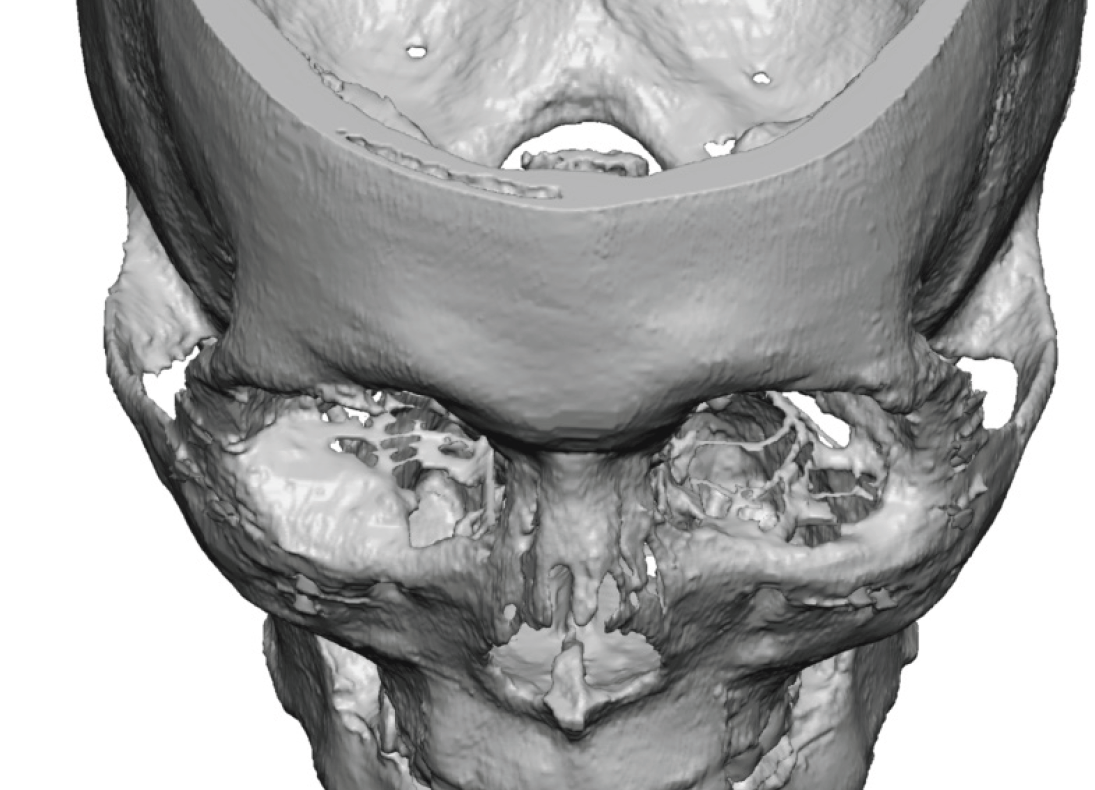


In vertical orbital dystopia (VOD) one eye sits lower than the other which is the direct result of a lower orbital floor and infraorbital rim. While it is uncommon that the lower bony floor of the eye is the only abnormal part of the hard and soft tissue orbital box and the resultant eye asymmetry, for the sake of this discussion we will assume that it is.
In budding up the orbital floor and infraorbital rim there are multiple materials which can be used to do so. These consist of autogenous bone can cartilage grafts to a variety of implant materials. One such implant is bone cement or, more specifically, hydroxyapatite bone (HA) cement. While the name may make one think it is a material that turns into bone, it does not and is best thought of as a bone-friendly implant material.

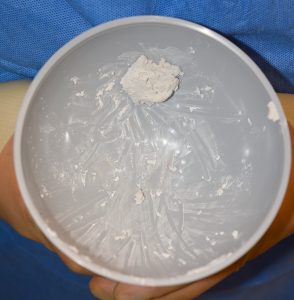 While there are many different manufacturers of HA bone cement they all consist of a liquid and powder which is mixed to create a putty consistency.
While there are many different manufacturers of HA bone cement they all consist of a liquid and powder which is mixed to create a putty consistency.

 Applying HA bone cement into the limited space of the orbital floor and rim acts much like a spackling material like plaster. It is applied as a thick paste and then shaped with instruments to the desired form. It takes about 10 minutes for the material to become fully set.During the mixing process antibiotic powder can be added to the cement for postoperative diffusion into the implant space.
Applying HA bone cement into the limited space of the orbital floor and rim acts much like a spackling material like plaster. It is applied as a thick paste and then shaped with instruments to the desired form. It takes about 10 minutes for the material to become fully set.During the mixing process antibiotic powder can be added to the cement for postoperative diffusion into the implant space.


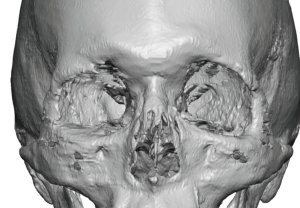
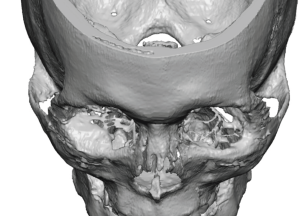 The bone cement can be seen in postoperative 3D CT scan due to its mineral content. Its effects are similar to any other implant material in which its lifting effect is related to how much material is added.
The bone cement can be seen in postoperative 3D CT scan due to its mineral content. Its effects are similar to any other implant material in which its lifting effect is related to how much material is added.
While HA bone cement is a ceramic implant materials, advantages are that it can be shaped into almost any form and acts biologically almost like bone. Its disadvantages are that it is a technique-sensitive material and requires a non-wet tissue environment for proper shaping and setting. In my experience it is best used when smaller amounts of orbital augmentation are required and the patient prefers a ‘non-implant’ material.
Dr. Barry Eppley
Indianapolis, Indiana