

Rib removal surgery is done for a variety of reasons. I divide indications for these ribcage modifications into aesthetic waistline narrowing, vertical waistline elongation and removal of asymmetries or anomalous rib lengths/shape. But no matter the indication for their removal the technique consists of opening the musculoperiosteal ‘tube’ in which it resides and removing it from there in.
Between the muscle and periosteal dissection off of the rib circumferentially as well as separating it from its bony and/or cartilaginous attachments, postoperative discomfort is to be expected. The typical intraoperative approach to postoperative pain management would be intercostal nerve blocks using with Marcaine or Exparel. But injecting in or around the nerve always risks injury to it and there is no assurance as to how much of the medication will stay where it can work best.
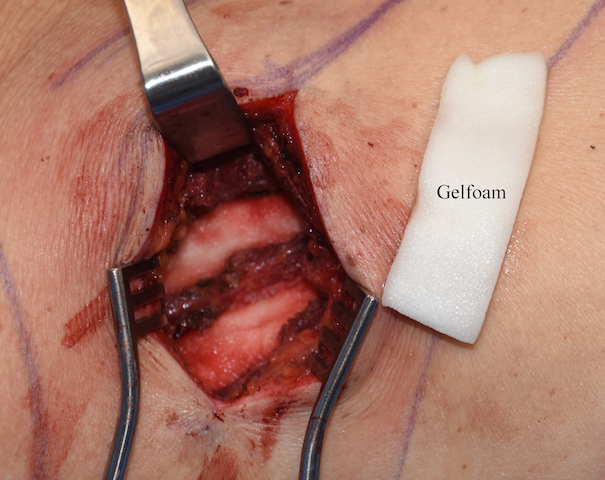
 A technique that I use in rib removal is to pack the void left by removal of the rib with gel foam sponges soaked in Exparel. Exparel is the long-acting local anesthetic that is commercially available to date. This provides a harmless application of sustained drug release along the whole length of the exposed intercostal nerve. The muscle is then closed over it for each individual rib removal site. The gelfoam holds onto the medication for days and perhaps as long as it takes for complete breakdown and absorption of the collagen-based sponge. (weeks)
A technique that I use in rib removal is to pack the void left by removal of the rib with gel foam sponges soaked in Exparel. Exparel is the long-acting local anesthetic that is commercially available to date. This provides a harmless application of sustained drug release along the whole length of the exposed intercostal nerve. The muscle is then closed over it for each individual rib removal site. The gelfoam holds onto the medication for days and perhaps as long as it takes for complete breakdown and absorption of the collagen-based sponge. (weeks)
The remaining amounts of Exparel solution is injected into the surrounding muscle layers above the excised rib sites and the skin incision as would normally be done.
While rib removal surgery is certainly not comfortable immediately after surgery, this application of a long-acting (72 hour) local anesthetic sponge technique helps patients feel less discomfort than they otherwise would. While many presume postoperative rib removal pain to be considerable, that has not been my observation.
Dr. Barry Eppley
Indianapolis, Indiana