

Treatment of very specific types of migraine headaches can be successfully done by extraforaminal decompression techniques. This is especially true for the migraine trigger site of the supraorbital nerve. By removing all of the muscle from around the neurovascular bundle (and occasionally removing some foraminal bone and ablating the artery) a decrease in the severity and frequency of migraine headaches can be potentially achieved.
But despite the procedure’s ultimate success at migraine reduction, very often migraine surgery creates an immediate postop migraine event. This is not surprising given the trauma that results in and around the nerve from its decompression. While such a migraine ‘reaction’ does not occur in every patient, it certainly is distressing to those in which it does. In the short term it is very much like ‘adding insult to injury’.
 Several intraoperative techniques can be useful for reducing the risk of an immediate after surgery migraine attack. After the induction of anesthesia, supraorbital nerve blocks are done using a 0.25% Marcaine and epinephrine (1:200,000) solution. (bupivicaine) This will block nerve sensations in the forehead and create a profound but temporary numbness of the supraorbital nerve’s anatomic distribution. These effects will wear off in 24 hours.
Several intraoperative techniques can be useful for reducing the risk of an immediate after surgery migraine attack. After the induction of anesthesia, supraorbital nerve blocks are done using a 0.25% Marcaine and epinephrine (1:200,000) solution. (bupivicaine) This will block nerve sensations in the forehead and create a profound but temporary numbness of the supraorbital nerve’s anatomic distribution. These effects will wear off in 24 hours.
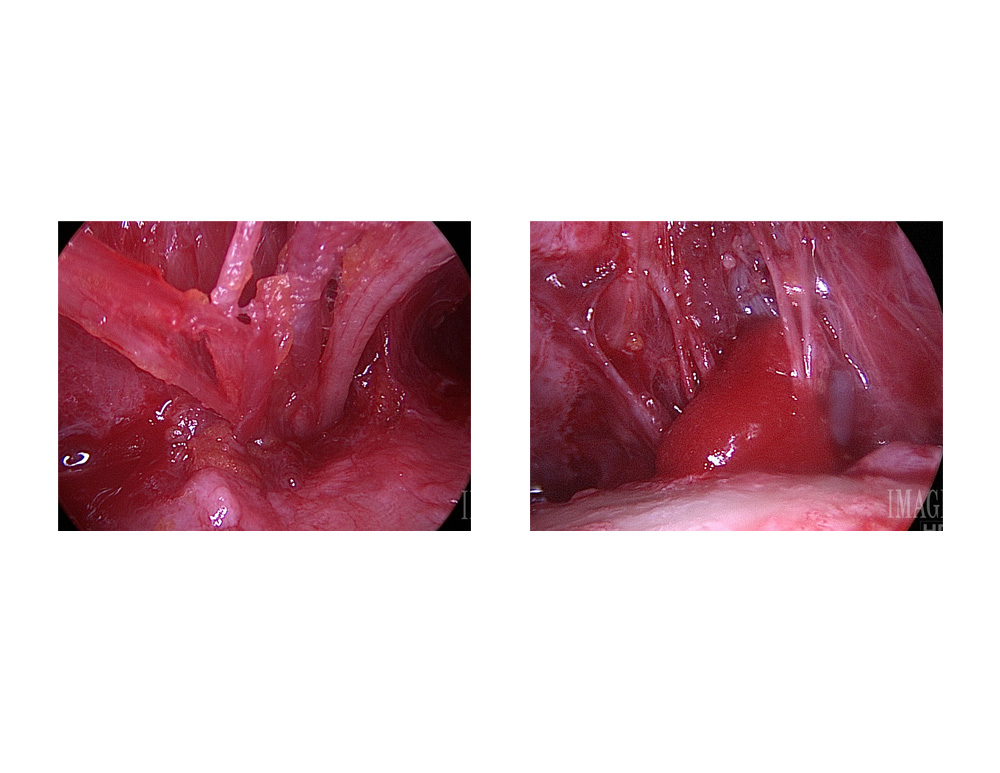 Another intraoperative technique is to treat the base of the supraorbital nerve with steroids after it has been decompressed. This is best done by soaking a dissolveable collagen sponge with Kenalog (triamcinolone) and wrapping it completely around the now visible nerve branches. This will have a calming effect on the nerve that will last well beyond that of the local anesthetic Marcaine.
Another intraoperative technique is to treat the base of the supraorbital nerve with steroids after it has been decompressed. This is best done by soaking a dissolveable collagen sponge with Kenalog (triamcinolone) and wrapping it completely around the now visible nerve branches. This will have a calming effect on the nerve that will last well beyond that of the local anesthetic Marcaine.
Dr. Barry Eppley
Indianapolis, Indiana